Introduction Demographics Causes Clinical features Complications Diagnosis Physical methods of hair removal Complications of physical methods of hair removal Medical treatment Prevention Outlook
Hirsutism is a male pattern of secondary or post-pubertal hair growth occurring in women. It arises in the moustache and beard areas at puberty when hair also appears in non-hirsute women in the underarm and pubic areas. Hirsute women may also develop thicker, longer hair than is usual on their limbs and trunk.
Hirsutism is also known as hirsutes.






Which women are considered hirsute varies according to culture and ethnicity, as the normal range of secondary hair growth varies with race. It should also be noted that women spend a great deal of time and energy removing unwanted hair, resulting in an unnaturally hair-free norm in today’s society.
Hyperandrogenism is often associated with polycystic ovaries, insulin resistance and obesity. Rare causes include:
Different genes expressed in individual hair follicles vary in their response to androgens.
Hirsutism is usually first noted in the late teenage years and tends to gradually get more severe as the woman gets older.
Hirsutism can involve a single site or multiple sites.
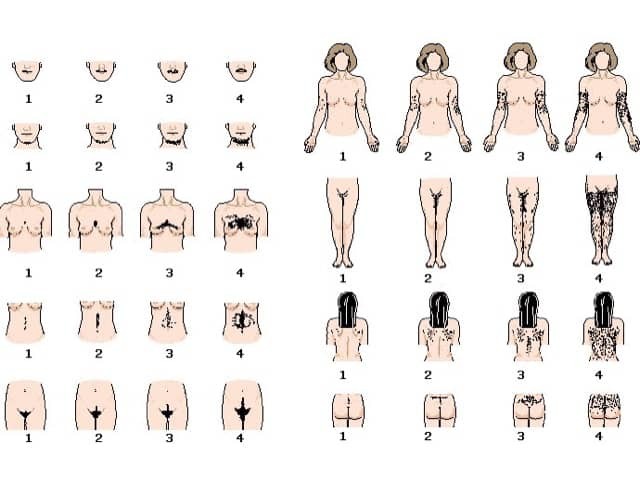
The severity of hirsutism is assessed using the Ferriman-Gallwey visual scale or a modified version, which assesses 9 areas of the body. The score varies from 0 (no hair) to 4 (extensive hair growth) in each area.
A general examination may reveal clues as to the cause of hirsutism.
Diagnostic features for polycystic ovary syndrome are:
People affected by excessive hair may suffer from great embarrassment with consequent psychosocial effects. They may go to considerable lengths and expense to remove the hair.
Other complications can arise from an underlying disease if any.
Hirsutism is diagnosed clinically. Investigations are not usually necessary unless the patient has a Ferriman-Gallwey score of > 15 when blood tests are done to evaluate male hormone levels and underlying diseases.
Free androgen index is total testosterone concentration divided by sex hormone binding globulin concentration and multiplied by 100. If elevated, check:
If early-onset of hirsutism, premature adrenarche, and/or family history of congenital adrenal hyperplasia:
If Cushingoid features:
If menstrual disorder:
General health:
A pelvic examination and abdominal/transvaginal ultrasound examination of the ovaries may be performed, as polycystic ovaries are a common cause of hirsutism.
Bleaching makes excessive hair less obvious.
Depilatory creams are generally based on thioglycolate (also used in perming solutions). A thick layer is applied for 15-30 minutes to the hairy area, then wiped off and the hair comes off with the cream. Depilatory creams can irritate and cause dermatitis.
Shaving, if necessary twice daily, will prevent unsightly stubble. Shaving does not make the hair grow more thickly.
Waxing needs to be repeated every six weeks. The warm wax hardens on the skin and as it is stripped off, the hairs are pulled out with it from the roots.
These remove the hair by a combined cut and pull.
Electrolysis or thermolysis may result in permanent hair loss but it takes time. A small probe is inserted along each hair, and a small electrical or heat discharge destroys the hair. A small area is treated every few weeks. It can be expensive if the area affected is extensive. Unskilled treatment may cause scarring.
Long wavelength lasers and intense pulsed light are the most effective devices for hair removal. This is mostly used for dark hair growing in white skin but dark hair in brown skin can also be treated by some centres. Expect multiple treatments over months to years.
Folliculitis is an unfortunate risk of plucking, shaving, and waxing. The treated hair follicles become inflamed, and painful pustules may develop.
Folliculitis may take weeks to settle. Hair removal has to be stopped, at least temporarily.



Women with the polycystic ovarian syndrome, particularly if they are overweight or have metabolic syndrome, may be prescribed metformin or rosiglitazone (more commonly used in type 2 diabetes).
Hormonal treatment using antiandrogen medicines (which counteract the male hormone) may be used for women with moderate or severe hirsutism. In many cases, the hair growth slows down and the hairs become thinner and less noticeable. It takes between six and twelve months to notice much difference, and then the medicine should be continued for several years.
Spironolactone 50-200 mg daily can slowly reduce excessive hair growth. It is sometimes combined with the oral contraceptive pill. Side effects include tender breasts and irregular menstrual bleeding.
Although several low dose combined birth control pills may be helpful, it is best to select one that has been specifically formulated to treat hirsutism. These contain oestrogen and antiandrogenic progesterone: cyproterone (co-pyrindiol, with trade names Diane™-35, Estelle™ 35, Gien™ 84), drospirenone (Yasmin™, Yaz™) or dienogest (Valette™). Side effects include spotting (bleeding between periods), tender breasts, nausea and headaches, especially in the first few months. The oral contraceptive pill is not suitable for everyone. Please refer to the New Zealand Ministry of Health (Medsafe) advice on the use of combined oral contraceptives.
Larger doses of cyproterone (50–200 mg for 10 days each cycle), are combined with the oral contraceptive pill and are very effective for most women with hirsutism. Side effects include weight gain, depression, and loss of libido. Specialist approval is required for prescription in New Zealand.
Hair removal creams containing eflornithine are available in some countries.
It is not yet possible to prevent genetically predetermined excessive hair growth. Insulin resistance associated with obesity can be reduced by weight loss and dietary control.
Prognosis depends on the cause. The most common types of excessive hair growth persist life-long. Hirsutism has a tendency to be more pronounced with age.

