What is immunohistochemistry?
Immunohistochemistry (IHC) is considered to be an advanced form of histopathology. Immunohistochemistry is not usually used initially but is added when routine/regular histological testing is insufficient to form a diagnosis.
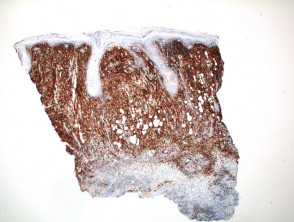
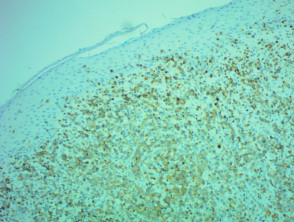
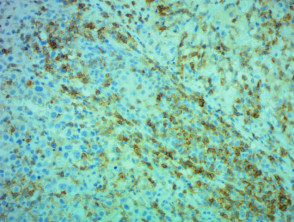
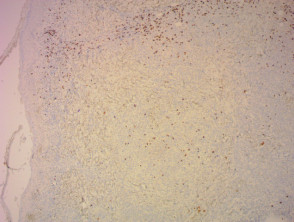
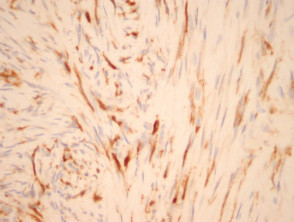
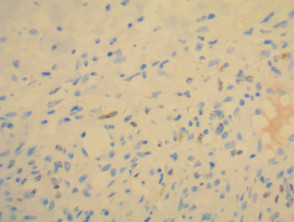
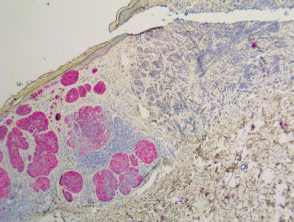
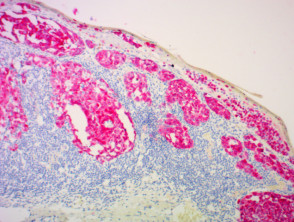
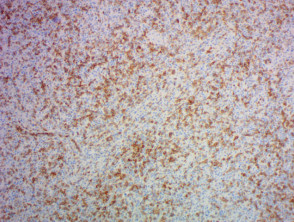
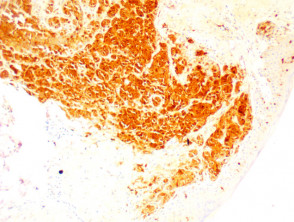
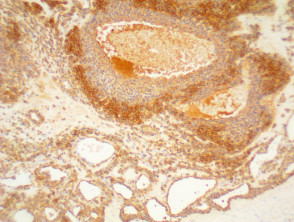
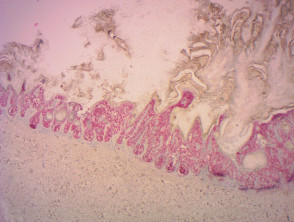
IHC uses primary antibodies to label a protein, then uses a secondary antibody which is bound to the primary one. In immunoperoxidase staining, an antibody is joined to an enzyme, peroxidase, that catalyses a reaction in which the protein is specifically stained brown. IHC can also involve fluorescently labelled antibody so that when viewed under a light microscope a certain pattern will be observed from the emitted fluorescence.
The IHC pattern is considered diagnostic, demonstrating nuclear, membranous or cytoplasmic patterns. IHC is often used in situations where a presence or absence of certain proteins can form a basis for a diagnosis. It can also be used to distinguish between two different disease processes that may otherwise appear similar to the pathologist.
How is immunohistochemistry performed?
The most common process of preparing immunohistochemical slides is as follows:
- Fixation of the tissue (in general, IHC stains are fixed with formalin)
- Embedding of the tissue (in paraffin)
- Sectioning of the tissues
- Retrieval (done with the application of heat or proteolytic enzymes)
- Mounting and dehydration
- Clearing and observation of the slides.
What are the advantages and disadvantages of immunohistochemistry?
The advantages of IHC include:
- It is possible to use fresh or frozen tissue samples for IHC.
- IHC is well-established and readily available.
- The cost of IHC is relatively low
- It has a fast turn-around time.
- Because no live infectious agents are involved, the risk to human health is minimal.
The disadvantages of IHC are as follows:
- IHC stains are not standardised worldwide.
- While the cost of the procedure is relatively inexpensive, the equipment needed to perform IHC is costly.
- Quantifying results is difficult.
- IHC is subject to human error. Well-trained personnel are paramount.
What are some examples of immunohistochemistry stains?
Hundreds of immunohistochemical stains are used to identify different tumours and other neoplasms. Just a few of the IHC stains used in dermatology are listed below.
| IHC Stain | Uses/Image caption |
|---|---|
| BCL2 | Used to distinguish between basal cell carcinomas and trichoepitheliomas |
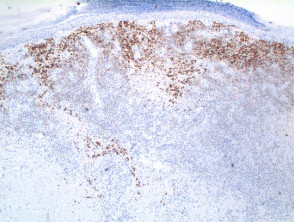
| CD3 | T-cell marker; strongly positive in mycosis fungoides |
| CD4 | Helper T-cell marker |
| CD8 | Suppressor T-cell marker |
| CD20 | B-cell marker |
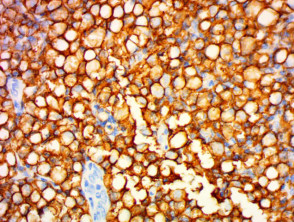
| CD30 | Can be used in the diagnosis of Hodgkin lymphoma and anaplastic lymphomas. Large cells: Golgi apparatus and membranous staining |
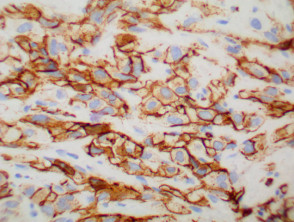
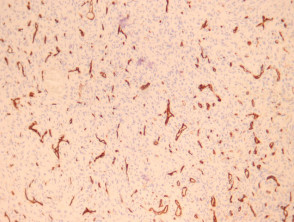
| CD31 | Helps to identify endothelial tumour |
| CD34 | Distinguishes different endothelial tumours and is positive in dermatofibrosarcoma |
| CD56 | Used in the diagnosis of non-Hodgkin lymphomas, leukaemias and small cell carcinomas |
| CD117 | Marker for KIT receptor and positive in various tumours including mastocytosis |
| CDKN2A (p16) | Tumour suppressor marker positive in HPV-associated tumours, actinic keratoses and squamous cell carcinoma |
| CK (various) | Cytokeratins can be used to help distinguish benign from malignant adnexal tumours |
| CK 20 | Specific for Merkel cell carcinoma. Can help identify adenocarcinomas of the gastrointestinal and reproductive system as well as gastrointestinal epithelial tumours |
| Cytokeratin High Molecular Weight | Used to detect ductal carcinomas, squamous cell carcinomas and other epithelial neoplasms |
| Desmin | Muscle marker |
| EMA | Used to identify eccrine neoplasms, Paget disease and sebaceous carcinomas |
| Factor 13 | Can help clinicians distinguish between dermatofibrosarcoma and dermatofibroma |
| HHV8 | Human herpesvirus 8 |
| HMB 45 | Used to detect melanocytes, especially in melanoma but negative in desmoplastic melanoma |
| Melan-a | Can help identify melanocytic naevus cells and melanomas |
| PDL1 | Programmed death-ligand 1 |
| S-100 | Used to mark tumours of the melanocytes, both naevi and melanoma |
| SMA | Smooth muscle antigen |
| SOX-10 | Nuclear marker for melanocytic tumours |
| Treponema pallidum | Demonstrates organisms in secondary syphilis |
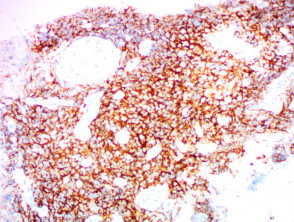
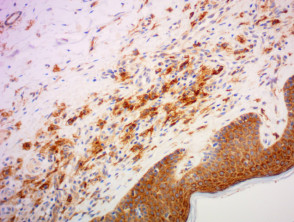
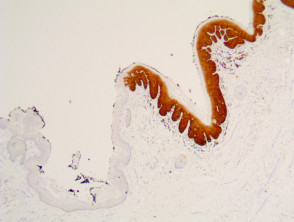
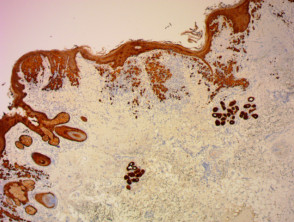
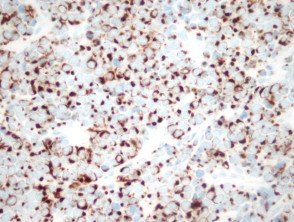
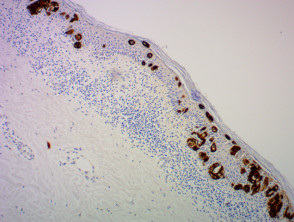
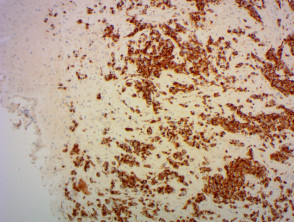
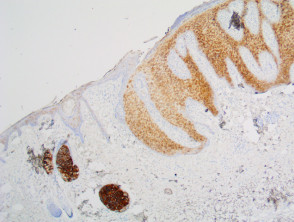
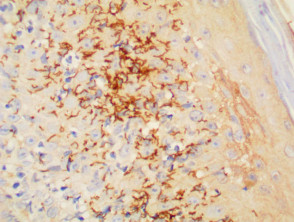
Immunohistochemistry stains