What is allergic contact dermatitis?
Allergic contact dermatitis is a delayed type hypersensitivity reaction in the skin following skin contact with an allergen [1].
What features are specific to children?
Allergic contact dermatitis is common in children because their skin can be easily sensitised. Compared to adults:
- Children’s skin is thinner
- Children's skin can absorb more applied substances
- Children have a higher surface area to body weight ratio
- Children are more likely to have underlying atopic dermatitis which facilitates sensitisation due to an impaired skin barrier [1].
Sensitisation mainly occurs in newborns and infants aged 0–3 years, and the prevalence of subsequent allergic contact dermatitis increases with age [1].
Allergic contact dermatitis in children



What causes allergic contact dermatitis in children?
Common allergens that trigger allergic contact dermatitis in children include:
- Nickel often related to piercings, buttons, fasteners, clips, toys, jewellery, and footwear [2]
- Myroxylon pereirae (Balsam of Peru) found in some fragranced products [2]
- Preservatives such as methylisothiazolinone and other isothiazolinones, particularly due to the use of baby wipes [2,3]
- Fragrance mix relating to the use of fragranced products [2]
- Colophonium found in adhesive tapes and musical instruments [2].
The relevant allergens in children vary with age. For example, allergic contact dermatitis caused by nickel is more common in adolescents than in newborns, as older children acquire piercings and wear jewellery and belts [3].
What are the clinical features of allergic contact dermatitis in children?
The clinical presentation of allergic contact dermatitis in children is similar to that in adults.
- When exposed to an allergen, the skin becomes red, itchy, and scaly within hours or up to a few days [4,5].
- The rash starts at the site of exposure to the allergen but may spread.
- There may be vesicles, blisters, and swelling [5].
- Common sites of allergic contact dermatitis in children include the hands, feet, arms, legs, and face [1].
- When the allergen is removed, the rash slowly resolves over several days to several weeks, but it will reappear with further contact with the allergen [4].
Rare morphologies, such as erythema multiforme, pigmented purpuric eruption, and pustular or granulomatous reaction patterns, are unlikely to occur in children because exposure to the allergens associated with these particular presentations is unlikely (eg, tropical woods, rubber diving suits) [4].
What are the complications of allergic contact dermatitis in children?
Allergic contact dermatitis in children can spread to cause a generalised rash (autoeczematisation) [5].
Systemic contact dermatitis is rare in children, with the most likely culprit being Myroxylon pereirae in food flavouring agents.
How is allergic contact dermatitis diagnosed in children?
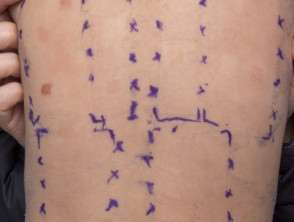
Allergic contact dermatitis is suspected clinically and is confirmed by patch testing. Patches containing the test substances are applied to the back for 48 hours, and the tests are assessed 48–96 hours later to identify the culprit allergen(s) [6]. Recently, the Australian Paediatric Baseline Series of 30 allergens was proposed, as compared to the larger Australian Baseline Series of 60 allergens [2].
Patch testing in children has a reasonable positive predictive value [2,7]. However, there may be false positives and false negatives [7,8]. It can be difficult to discriminate between irritation caused by the tested substances and weak allergic positive patch tests [7].
Patch tests

What is the differential diagnosis for allergic contact dermatitis in children?
As in adults, other conditions that can look similar to allergic contact dermatitis should be considered in children. These can include the following.
- Irritant contact dermatitis (eg, napkin dermatitis). Irritant contact dermatitis may be clinically difficult to differentiate from allergic contact dermatitis. It may be associated with dry and peeling skin, or very rarely, bullous eruptions. It is often well demarcated and rarely spreads to other areas [4].
- Atopic dermatitis. The characteristic distribution of atopic dermatitis involves the flexures. Secondary bacterial infection often occurs in children [4].
- Fungal infection (tinea). Tinea presents with one or more asymmetric annular, scaly plaques, which are not very itchy.
- Psoriasis. Psoriasis is usually symmetrical with well circumscribed erythematous and scaly plaques.
What treatment is available for children with allergic contact dermatitis?
The most important aspect of management is to identify the causative allergen. This may be obvious from the history or it may be necessary to perform patch testing.
- Allergic contact dermatitis is generally treated by the application of a mid-potency topical corticosteroid, with hydrocortisone used for the face [5].
- If the dermatitis is widespread, a systemic steroid (usually oral prednisone) is appropriate for several days followed by weaning [5].
- A topical calcineurin inhibitor may be considered for secondline treatment, especially with facial involvement [5].
Treatments, including emollients, should contain as few allergens as possible, since preservatives are a common cause of allergic contact dermatitis [5,6].
Allergic contact dermatitis has been reported to result in psychological effects in carers as well as in the affected child, inducing anxiety and depression. Therefore, psychological support should also be considered [3].
Counselling regarding allergen avoidance strategies is essential.
- The parents as well as the child may need to avoid the allergen (such as perfume).
- Exposure in newborns tends to occur from skin-to-skin contact from the parent, rather than directly to the allergen [1].
- Educate school-aged children to minimise exposure to the relevant allergen.
- Inform teachers to ensure that the child is not exposed to the allergen when parents are not present [6].
What is the outcome for children with allergic contact dermatitis?
As with adults, once sensitised, contact allergy may persist, so skin contact with culprit allergens should be avoided lifelong [4].