Introduction
Glomangiomas (also called glomuvenous malformation) differ clinically from glomus tumors in that they occur in childhood and adolescence, are usually asymptomatic, do not have a predilection for the subungal region, and often are multifocal. They can vary in colour from pink-to-blue and often become darker with age; they may be plaque-like or nodular. Multiple glomangiomas are rare and comprise about 10 percent of all glomus tumours.
Histology of glomangioma
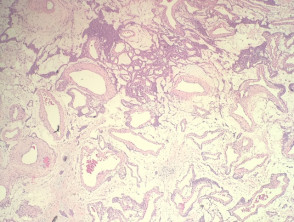
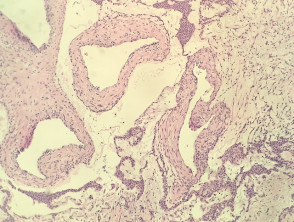
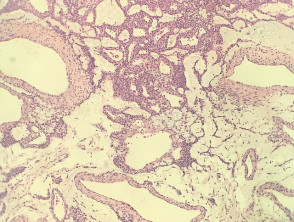
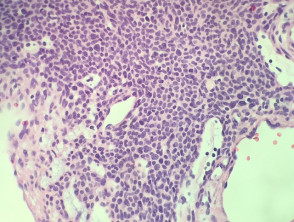
In glomangioma, the histopathology shows dilated venous channels that resemble venous malformations (figures 1, 2). Unlike venous malformations, they demonstrate single to multiple rows of surrounding cuboidal glomus cells (figures 3,4).
Glomangioma pathology
The glomus cells stain positively for vimentin and α-smooth-muscle actin but are negative for desmin, von Willibrand factor, and S-100.
Differential diagnosis for glomangioma
Other diagnoses to be considered include:
- Vascular malformation — these don't have the perivascular glomus cell accumulations seen in glomangioma
- Myopericytoma, angioleiomyoma, myofibroma — these all have varying degrees of perivascular muscle cells but these cells lack the classic cuboidal glomus cells. These tumours usually show a degree of desmin positivity in the perivascular cells which are not seen in glomangioma.