Orofacial granulomatosis is also referred to as granulomatous cheilitis, and is characterised clinically by chronic/relapsing swelling of the lips and oral mucosa.
Histology of orofacial granulomatosis
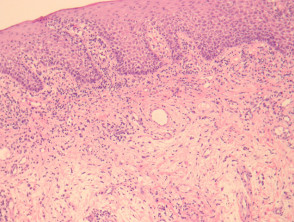
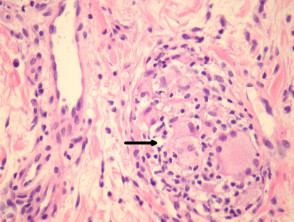
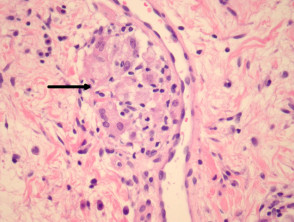
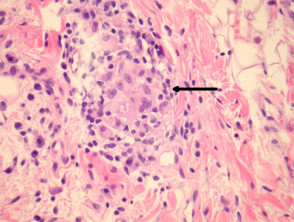
In orofacial granulomatosis, sections show oral mucosa with a sparse inflammatory infiltrate and mild oedema (figure 1). Higher power examination shows ectasia of lymphatics next to rare loose granulomas (figures 2-4, arrows indicate granulomas). Sometimes the granulomas may be difficult to find and extensive serial sectioning of the biopsy is recommended.
Orofacial granulomatosis pathology
Special studies of orofacial granulomatosis
Special stains for microorganisms may be performed to rule out an infection, given the granulomatous nature of the infiltrate.
Differential diagnosis of orofacial granulomatosis
Melkersson-Rosenthal syndrome: Shows the exact same pathology but clinically also shows facial nerve palsy and a “scrotal” tongue.
Crohn disease: Oral involvement with Crohn disease will be histologically identical. Clinical correlation is needed.
Sarcoid: Sarcoidal granulomas tend to be more overt and larger but some cases can be difficult/impossible to distinguish from orofacial granulomatosis.