What is Rothmund–Thomson syndrome?
Rothmund–Thomson syndrome is a rare inherited disease that affects the skin, eyes, bones and internal organs. At least 300 cases have been reported in medical journals since a case was first described by Rothmund in 1868. Rothmund–Thomson syndrome is also known as poikiloderma congenitale.
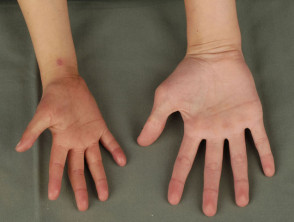
Rothmund–Thomson syndrome





What is the cause of Rothmund–Thomson syndrome?
Rothmund–Thomson syndrome is due to a genetic defect, in which there are mutations in the RECQL4 gene on Chromosome 8. This gene encodes for the enzyme DNA helicase which unwinds DNA (deoxyribonucleic acid). The abnormal gene makes the chromosomes unstable, altering the growth of cells in many tissues.
The defect is inherited as an autosomal recessive trait. This means an abnormal gene must come from each parent.
What are the clinical features of Rothmund–Thomson syndrome?
Affected children may be identified early in life by their small size, their tendency to sunburn easily, and from the appearance of their skin, teeth and bones. Rothmund–Thomson syndrome is slightly more common in females than males.
Skin
- Photosensitivity: sunburn-like redness, swelling and blisters on cheeks and face; may extend to involve buttocks and extremities. Noted during the first year of life in 90%
- Poikiloderma: variegated pigmentation, telangiectasia (prominent tiny blood vessels) and skin thinning; usually evident on cheeks, hands and buttocks by 3-5 years of age
- Thin eyebrows and sparse scalp hair
- Abnormal, brittle nails
Eyes
- Cataracts: lens opacities occur in 50% of children aged 3-7 years and are often bilateral.
- Corneal lesions are less common.
Bones
- Bony defects affect over 50% of children, who are often of short stature.
- These include dysplasia (abnormal growth), sclerosis (thickening and hardening) and cystic abnormalities of the long bones.
- Small hands and feet; absent or malformed radii and thumbs
- Osteoporosis and bone hypoplasia (bone thinning) are common with ageing. Pathological fractures may occur with minimal trauma.
- Other changes include widened long bone epiphyses (part of the bone where growth occurs), iliac bone hyperplasia (excessive growth), trabeculated metaphyses (middle part of the long bone).
Dentition
- Agenesia (absent formation of teeth)
- Microdontia (small teeth)
- Delayed and ectopic eruption of teeth
- Supernumerary teeth
Reproductive system
- Hypogonadism in 25%
- Juvenile-appearing genital organs
- Amenorrhoea (lack of menstruation)
- Sterility
Endocrine system
- Parathyroid adenoma
- Disturbed thyroid function
Gastrointestinal system
- Chronic nausea and vomiting
- Diarrhoea
Intellect
- Intellectual impairment in up to 30%
What are the complications of Rothmund–Thomson syndrome?
The main concern in Rothmund–Thomson syndrome is an increased susceptibility to cancer.
Skin cancer
Skin cancers including basal cell carcinoma, squamous cell carcinoma and intraepidermal carcinoma (Bowen disease) are common in older children and adults with Rothmund–Thomson syndrome. They often arise on the face, neck and limbs. It is postulated that skin cancers occur because of defects in DNA repair after exposure to ultraviolet radiation.
Bone cancer
The second most common type of cancer is osteosarcoma, which may develop in late childhood or adolescence. Osteosarcoma may arise within pre-existing bone dysplasia so it may be difficult to diagnose on X-ray.
Treatment of osteosarcoma in Rothmund–Thomson syndrome is similar to in patients without the syndrome.
Other malignancies
Other cancers affecting individuals with Rothmund–Thomson syndrome include:
- Gastric adenocarcinomas
- Fibrosarcomas
- Hodgkin lymphoma
- Malignant eccrine poroma.
Management of Rothmund–Thomson syndrome
Children with Rothmund–Thomson syndrome are often followed up by a paediatrician, dermatologist, orthopaedic surgeon, dental surgeon and/or other specialists. Clinicians should bear in mind the risk of cancers and should monitor and investigate as appropriate.
Sun protection is very important because of photosensitivity and increased risk of skin cancer. This should include seeking shade, fully covering clothing and broad-spectrum sunscreens.
Genetic counselling is important for family members.