Introduction
Dermoscopy is a non-invasive technique used to examine skin lesions with a dermatoscope. It is also known as dermatoscopy, epiluminescence microscopy, incident light microscopy, and skin-surface microscopy [1,2].
A dermatoscope usually consists of a light source, achromatic lens, contact plate, and power supply. A dermatoscope allows better visualisation of deeper skin structures, therefore improved diagnostic accuracy of skin lesions.
There are three main modes of dermoscopy [1,2]:
- Polarised contact dermatoscopy
- Polarised noncontact dermatoscopy
- Nonpolarised contact dermatoscopy (also called unpolarised dermoscopy).
Polarised and nonpolarised dermoscopy are complementary and the combination of both methods increases diagnostic accuracy and clinician confidence.
What are the physics of dermoscopy?
To understand the difference between the different modes of dermoscopy, it is important to know the basic physics of light, refraction, and reflection.
Reflection and refraction


A light wave is an electromagnetic wave; it can be thought of as an oscillating form that vibrates in multiple directions.
- Nonpolarised light is a light wave that vibrates in more than one plane.
- Polarised light vibrates in a single plane.
Polarised and nonpolarised light and polarisation

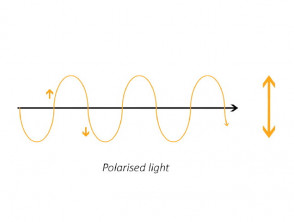

The process of transforming nonpolarised light to polarised light is known as polarisation.
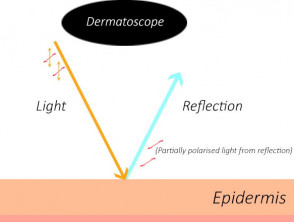
Most light sources, such as the sun, lamps, and torches, are nonpolarised. As the light hits the surface of the skin, it is absorbed, refracted, and reflected. Nonpolarised light can undergo polarisation by reflecting off nonmetallic surfaces, creating specular reflectance (glare). Glare reduces the ability of our eyes to see the underlying structures.
- Nonpolarised dermoscopy uses a glass plate as a medium with a smaller refractive index to skin to minimise glare [1,2].
- An interface fluid (such as alcohol, liquid paraffin, water, or ultrasound gel) is applied for contact dermoscopy. Interface fluid increases the penetration of light and allows excellent visualisation of the superficial layers of the skin from the epidermis to the dermo-epidermal junction [2].
- Polarised dermatoscopy uses cross-polarisation to view the structure. Two filters are held orthogonally at 90 degrees. The source light initially is polarised with the first filter, then the reflected light from the skin is blocked by the second filter. This technique minimises glare and allows better visualisation of the underlying structures, from the dermo-epidermal junction to the superficial dermis [1,2].
Nonpolarised and polarised dermatoscopy


What are the clinical differences between polarised and nonpolarised dermoscopy?
Different modes of dermoscopy produce similar results. However, there are minor differences in the appearance of cutaneous structures and colours [3]. Skin structures with high concordance between polarised and nonpolarised dermoscopy (described using conventional pattern analysis) include [4]:
- Leaf-like structures, ulcerations, fuzzy streaks, dots, globules, spoke-wheel areas, concentric areas, structureless areas, and blue-grey ovoid nests
- Brown, white, and blue-grey structures in basal cell carcinoma (BCC).
Structures with lower concordance between polarised and nonpolarised dermoscopy include [4]:
- White shiny structures, shiny white areas, and rosettes in BCC
- The pink–red of BCC.
Effect of polarisation in dermoscopy of pigmented basal cell carcinoma


See more images of polarised and nonpolarised light in dermoscopy images.
The depth of visualised structures
Polarised dermoscopy can be used to view deeper layers (the dermo-epidermal junction and superficial dermis).
Nonpolarised dermoscopy is used to view superficial layers (the superficial epidermis to the dermo-epidermal junction).
Contact
Polarised dermoscopy does not require skin contact or fluid immersion.
Nonpolarised dermoscopy always requires skin contact and fluid immersion.
Colours and structures
Polarised dermoscopy is better at showing variable pigmentation, dermal vessels, pink/red colours, and white shiny structures.
Effect of polarisation in dermoscopy of pigmented basal cell carcinoma


Nonpolarised dermoscopy is better at showing blue-white colours, peppering, milia-like cysts, and comedo-like openings.
Effect of polarisation in dermoscopy of seborrhoeic keratosis


On the palms and soles, nonpolarised dermoscopy is better at showing eccrine duct openings and pigment in the furrows.
Effect of polarisation in dermoscopy of acral melanocytic naevus


Diagnostic accuracy
Polarised dermoscopy has increased sensitivity for detecting amelanotic melanoma or structure-poor melanoma and basal cell carcinoma.
Effect of polarisation in dermoscopy of amelanotic melanoma


Polarised dermoscopy is better at visualising dermatofibroma, BCC, some cases of melanoma, and squamous cell carcinoma (SCC).
Effect of polarisation in dermoscopy of dermatofibroma


Effect of polarisation in dermoscopy of superficial basal cell carcinoma


Effect of polarisation in dermoscopy of pigmented melanoma


Nonpolarised dermoscopy has increased specificity for seborrhoeic keratosis and is better at visualising acral lesions.
Effect of polarisation in dermoscopy of seborrhoeic keratosis


Either method can be used to diagnose most skin lesions; they provide complementary information.