Introduction
Lichen aureus is a distinct subtype of pigmented purpuric dermatosis. Clinically, it usually effects children or young adults and presents as persistent rust-coloured plaques on the lower extremities.
Histology of lichen aureus
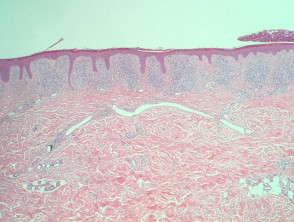
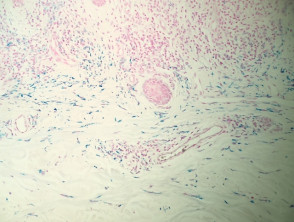
In lichen aureus, sections typically show a distinct pattern of infiltration in all types of pigmented purpuric dermatitis, with infiltration around the small vessels of the superficial plexus and minimal epidermal reaction (figure 1). At higher power, the infiltrate is mainly composed of lymphocytes with quite an impressive proportion of histiocytes (figure 2). The vessels may have some prominence of the endothelial cells but there is no evidence of vascular damage. A key feature of all types of pigmented purpuric dermatitis is the presence of haemosiderin within the superficial dermis, which results from chronic leakage of red blood cells from the vessels.
Lichen aureus pathology

Special studies for lichen aureus
Perls' Prussian blue iron stain demonstrates the deposition of haemosiderin in the superficial dermis (figure 3).
Differential diagnosis for lichen aureus
Other diagnoses to be considered include:
- Other forms of pigmented purpuric dermatitis — some authorities no longer make the distinction between the clinical forms of pigmented purpuric dermatitis; histopathologically, lichen aureus has a high percentage of histiocytes in the infiltrate
- Histiocytic disorders (eg, Langerhans cell histiocytosis) — these can be excluded by demonstration of dermal haemosiderin with Perls' iron stain
- Mycosis fungoides — pigmented purpuric dermatitis can on occasion mimic cutaneous T-cell lymphoma histopathologically; dense histiocytic infiltrates and dermal haemosiderin are unusual in mycosis fungoides
- Leukocytoclastic vasculitis — this shows convincing vessel damage with neutrophilic infiltration and fragmentation.