Introduction
Neurocristic hamartoma presents as a slowly enlarging multinodular variably pigmented plaque. It most commonly presents in the head and neck region but has been described arising in a diverse range of sites. Malignant transformation is a well-described complication.
Histology of neurocristic hamartoma
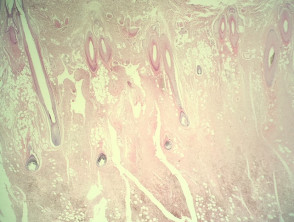
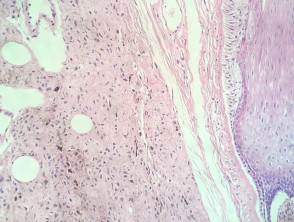
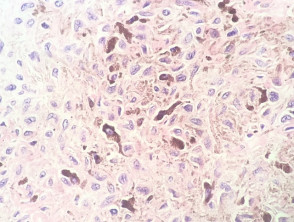
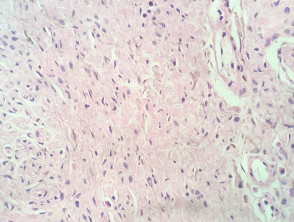
In neurocristic hamartoma, the histopathology shows a lesion composed of various components of neural crest origin, typically melanocytes, stroma and peripheral nerves. Low power examination shows a lesion which extends deep in to the dermis, involves the subcutis (figure 1), and surrounds the hair follicles (figure 2). Closer examination shows areas with epithelioid melanocytes with heavy pigmentation (figure 3). In other areas there is a mixture of fibrous areas and peripheral nerve differentiation. Sometimes, the epithelioid areas can show a degree of nuclear atypia and even frankly malignant nuclear changes.
Neurocristic hamartoma pathology
Special studies for neurocristic hamartoma
Immunohistochemistry demonstrates that the areas with melanocytic differentiation are positive with Melan-A, S100 and often with HMB-45. The neural areas are negative with Melan-A and HMB-45 but show S100 reactivity. Fibrous regions of the lesion are negative for all of these markers.
Differential diagnosis for neurocristic hamartoma
Other diagnoses to be considered include:
- Congenital naevus — these will not show the mixture of nerve and fibrous tissue and typically lack the heavily pigmented epithelioid component
- Plaque-type blue naevus — some authorities regard this as being the same lesion. Fibrous and neural differentiation may not be seen in this variant of blue naevus
- Melanoma — expansile growth and marked nuclear atypia in neurocristic hamartoma mimic melanoma. Malignant transformation is a well described phenomenon in neurocristic hamartoma with the metastatic deposit being very difficult to distinguish from regular melanoma or malignant blue naevus.