Created 2008.
Note: dermatoscopic images in this course are nearly all at the same magnification; the full width of the image is equivalent to 12 millimetres on the patient.

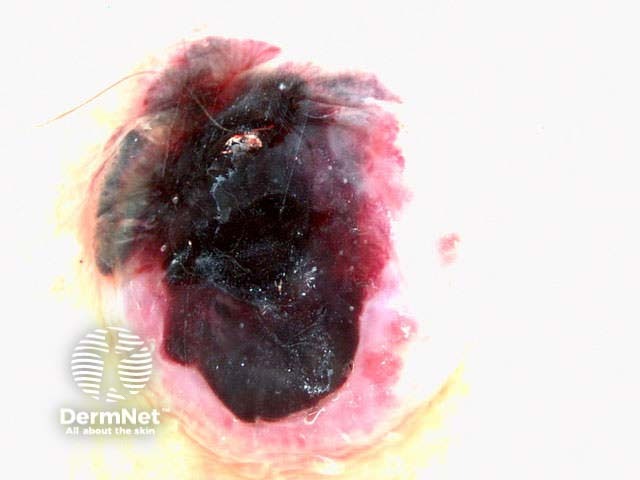
By dermoscopy, the pigmentation of the lesion is evaluated in terms of colour(s): black, dark brown, tan, grey, steel blue, purple, white, yellow and red.







Clinically, symmetry may be evaluated in terms of shape. Symmetry of shape suggests a benign lesion, and asymmetry suggests melanoma (the ‘A’ and ‘B’ of the American ABCDE's). However, an odd-shaped lesion may also be benign.




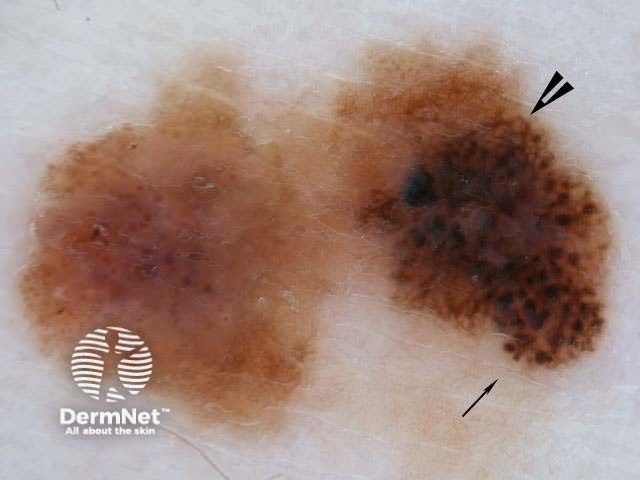
By dermoscopy, symmetry is evaluated in terms of pigment pattern (colour and/or structure). Symmetrical pigment pattern is typical of benign skin lesions. Complete asymmetry suggests the lesion may be malignant, but may also be seen in some atypical naevi.
Uniform pigment may also be called ‘homogeneous’ (benign), and an irregular pattern may be called ‘heterogenous’ (atypical or malignant).




Melanocytic lesions are made up of three types of structure.
Benign lesions tend to have only one or two of these structural patterns in a symmetrical distribution. Malignant lesions tend to have areas of network, amorphous structures and scattered globules in an atypical distribution.
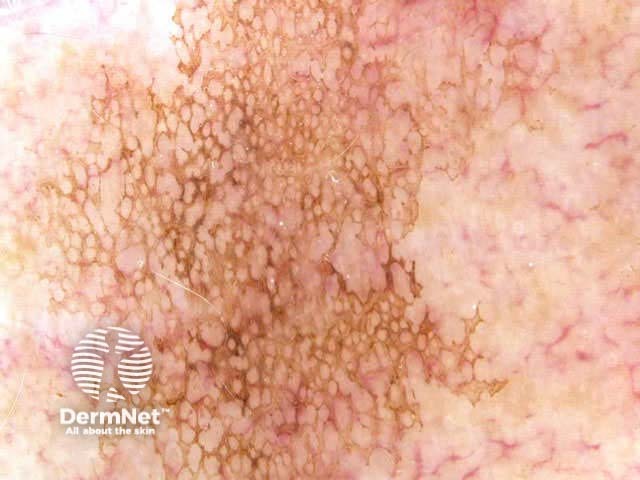
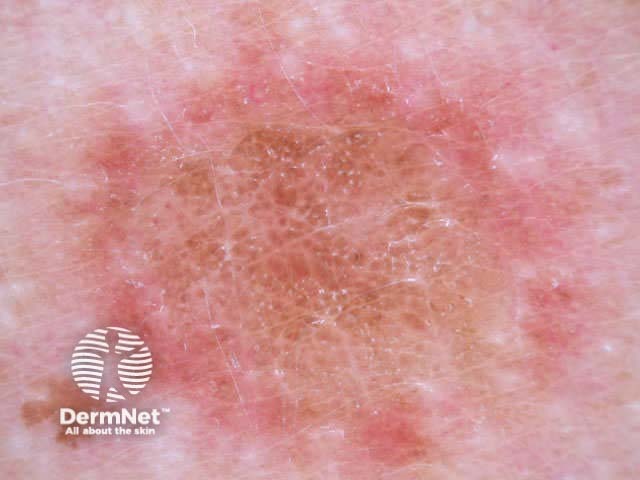
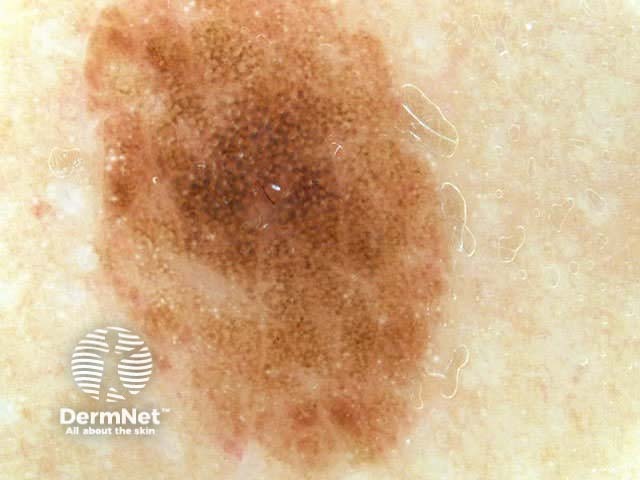
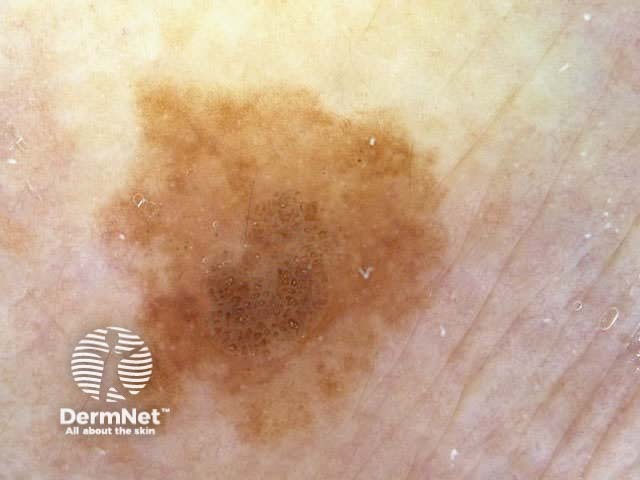
Pigment network is formed by melanocytes or melanin in basal keratinocytes. Dense pigment rings (the grid) are due to projections of rete pegs or ridges. The paler ‘holes’ are due to projections of dermal papillae.
A fine regular network is seen in some typical and atypical benign melanocytic lesions. In some sites the network is widened (larger ‘holes’). It does not have to occupy the whole lesion.











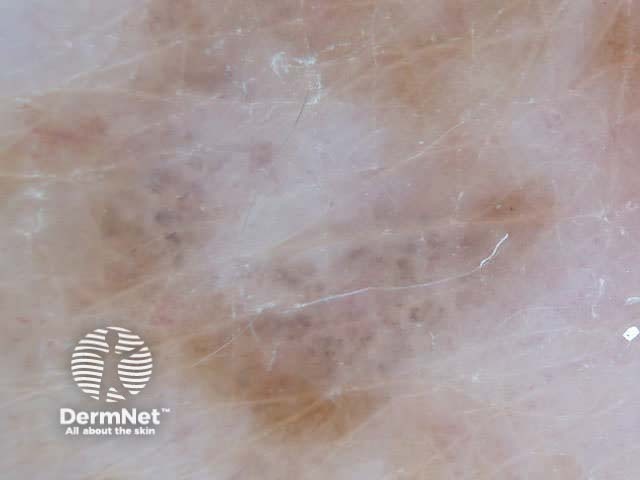
The term ‘pseudonetwork’ is used when annular pigmentation is seen around hair follicles on facial skin. At times on the face, it may be difficult to differentiate benign naevi, lentigo, actinic keratoses, lichenoid keratosis and early lentigo maligna.

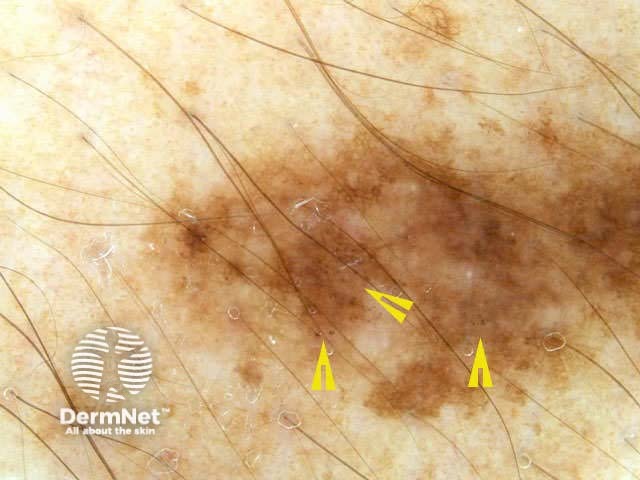
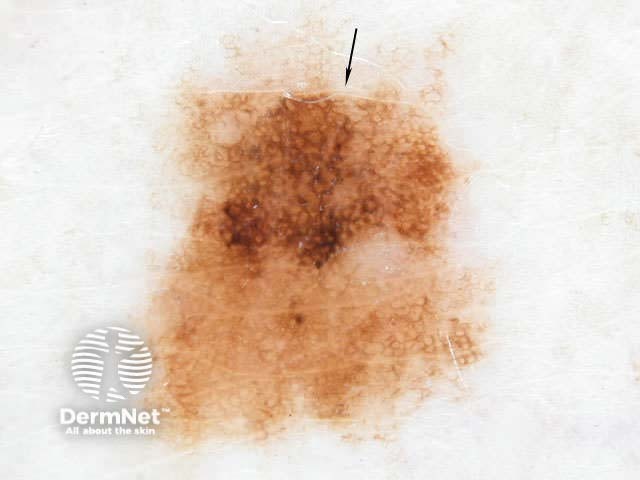
An atypical or irregular pigment network may be found in atypical or dysplastic naevi and some melanomas.




‘Negative pigment network’ refers to a white reticular pattern due to elongated rete pegs. It is a characteristic of melanoma but also sometimes seen in Spitz naevi and some dysplastic naevi. It may resemble the pattern seen in scars on the lower leg (atrophie blanche). It should not be confused with the pale colour separating the globules of a benign naevus.


‘Parallel pattern’ refers to the network seen within most melanocytic naevi on palmar and plantar surfaces. It may be helpful to apply ink to the skin surface and then wipe it off, which reveals the furrows.
There is no obvious parallel pattern in homogenous-type naevi on volar sites.








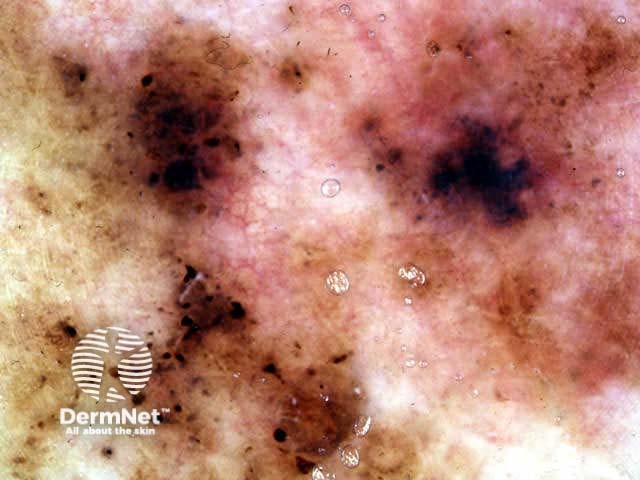
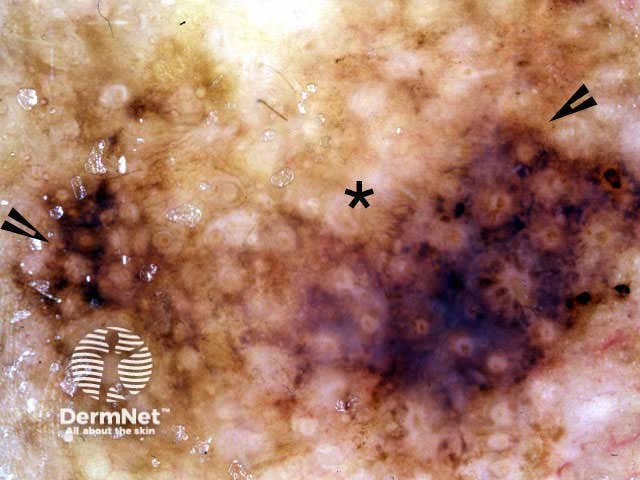
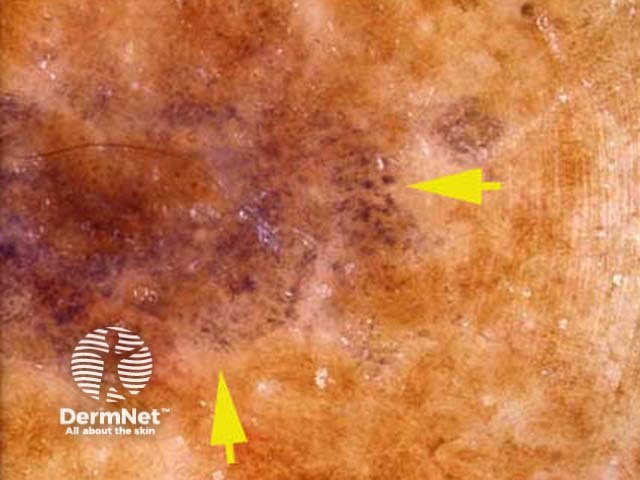
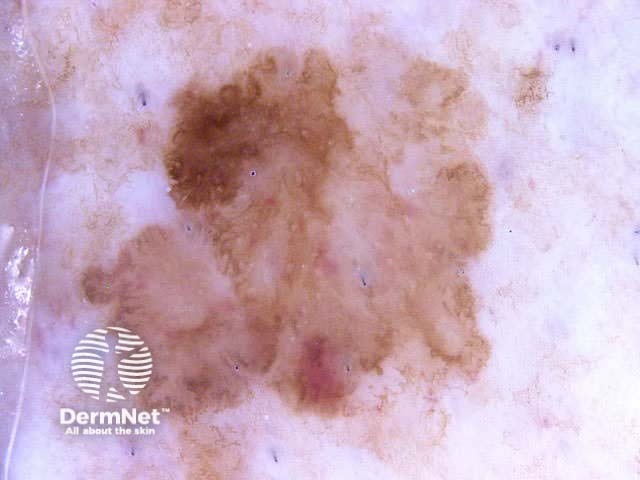
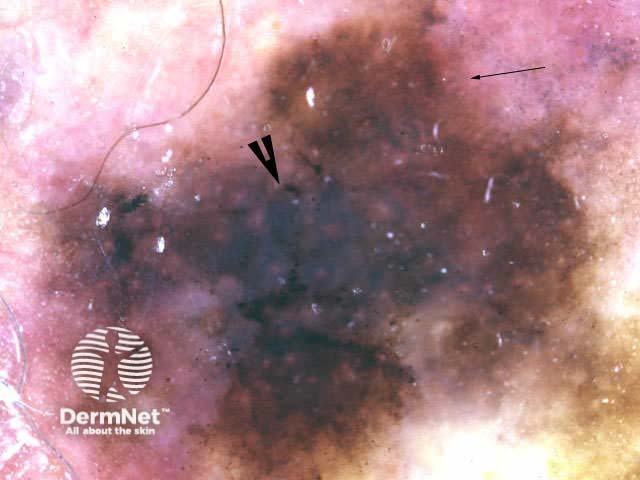
Diffuse pigmentation without specific structural features is variously described as amorphous areas or blotches.
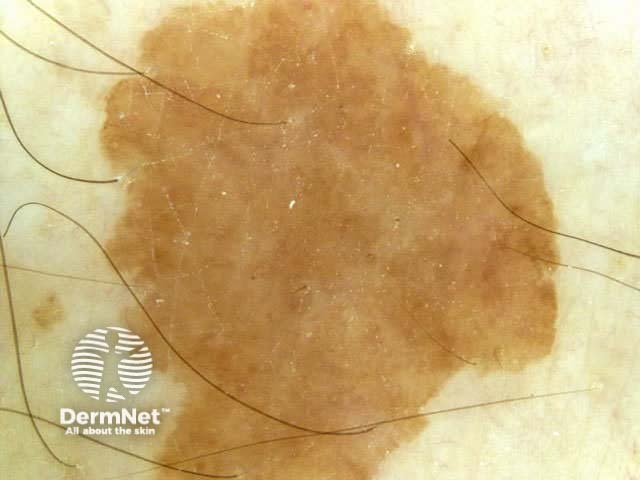

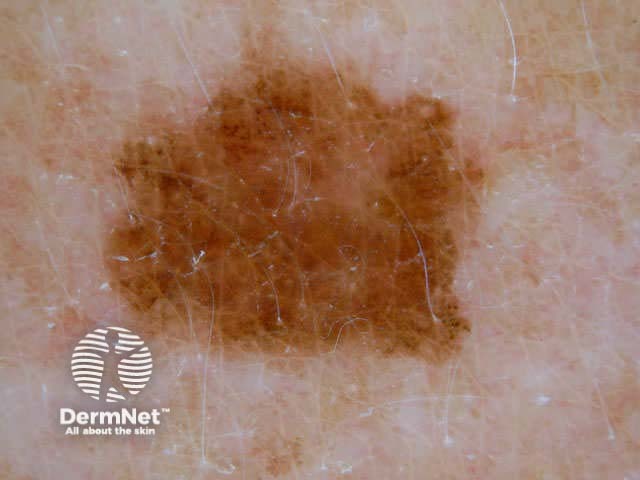
Irregular blotches are sometimes the only dermoscopic feature of melanoma. They may also arise in dysplastic naevi.



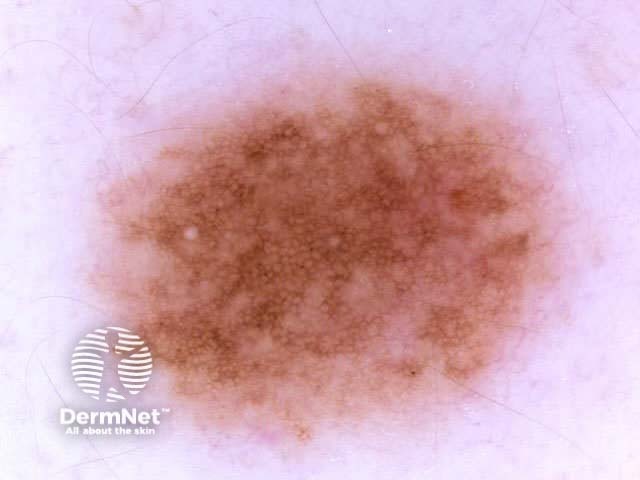
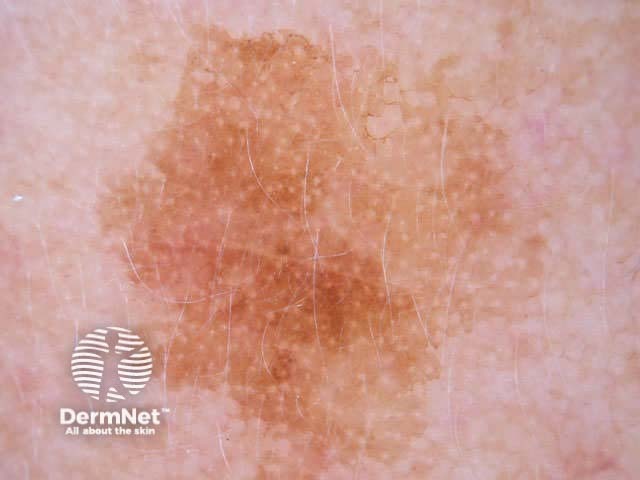
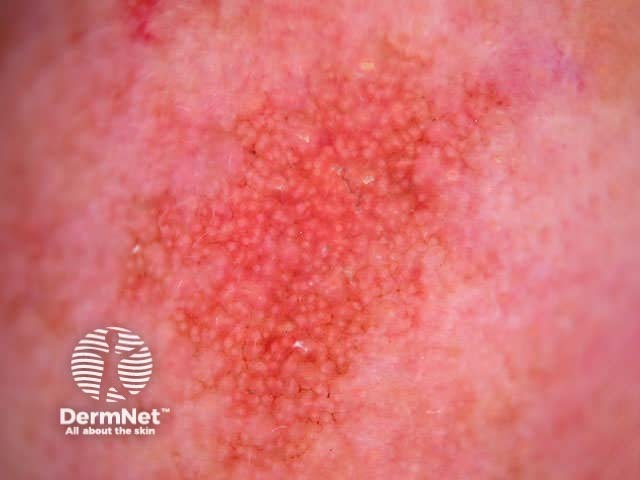
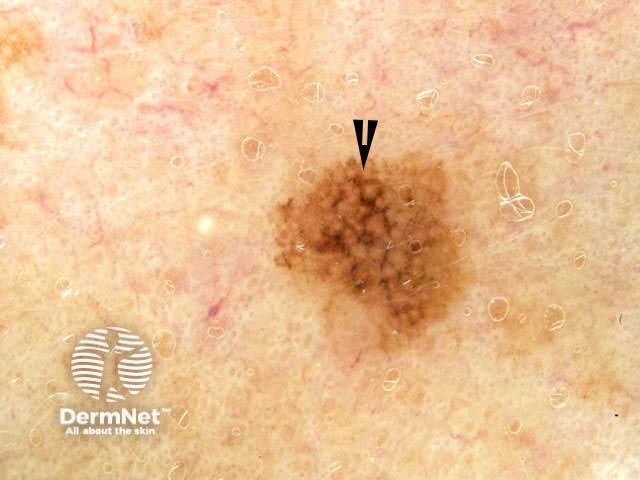
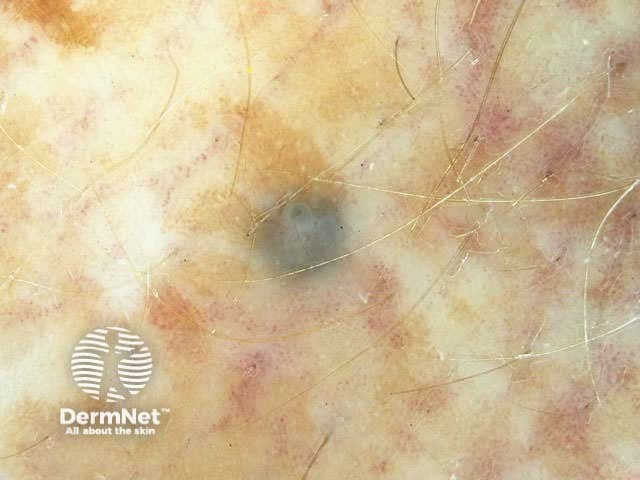
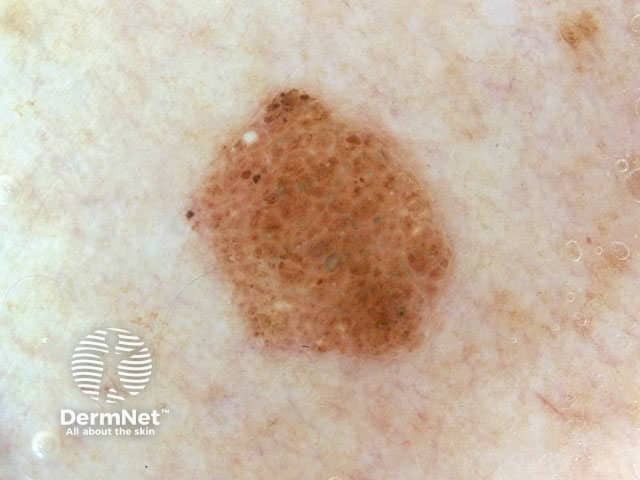
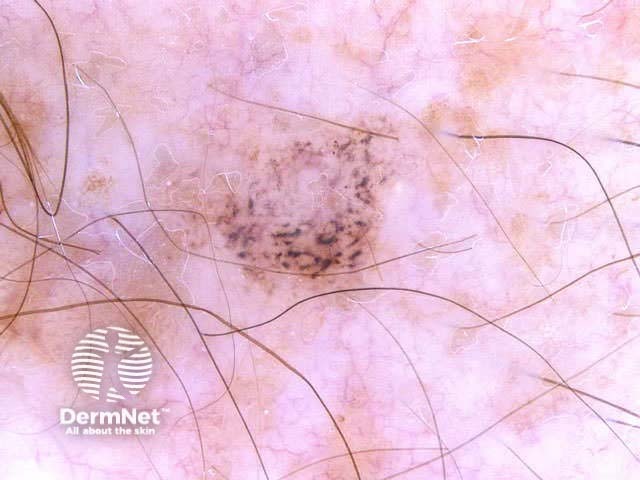
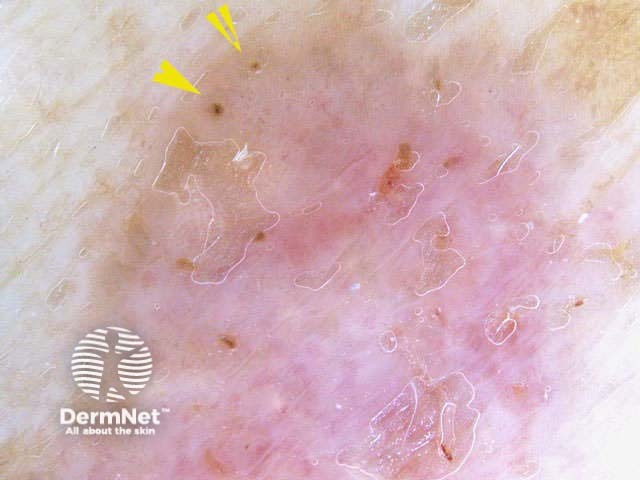
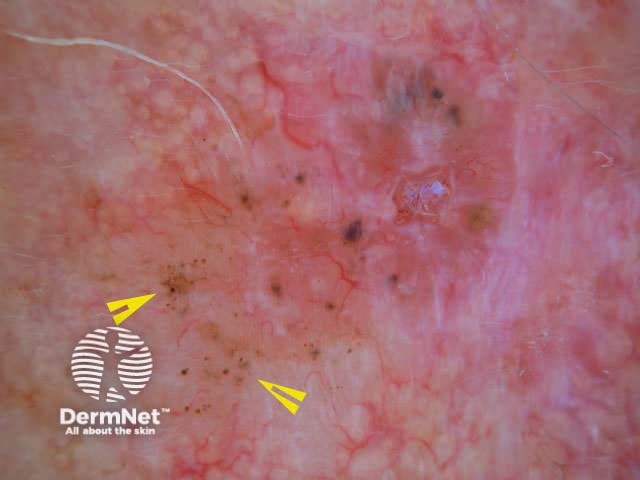
Globules are large dots. Dots and globules represent localised pigment. The colour determines their site: black dots are due to free melanin in the stratum corneum, brown globules are due to junctional nests of melanocytes, and blue or grey dots are due to melanophages in the dermis.







Dots may be seen in pigmented basal cell carcinoma and rarely in seborrhoeic keratoses.


Some specific dermoscopic structures are helpful in the diagnosis of non-melanocytic lesions. These include:
Leaf-like areas are grey, brown or blue shiny, discrete bulbous structures unassociated with a pigment network (structureless). They are seen on the edges of pigmented basal cell carcinoma, when they often have darker areas within them (blue ovoid masses). Some may not appear very like a leaf, in which case they are better known as ‘structureless areas’. The moth-eaten edges of solar lentigos also sometimes appear leaf-like.



Blue ovoid masses are large discrete pigmented round, oval or bullet-shaped blue structures and are characteristic of basal cell carcinoma. When the structure has radial projections, they are called ‘spoke-wheel areas’. They are often found within leaf-like or structureless areas. Blue blotches that are sometimes seen in melanoma are irregular, less well defined and appear out of focus.



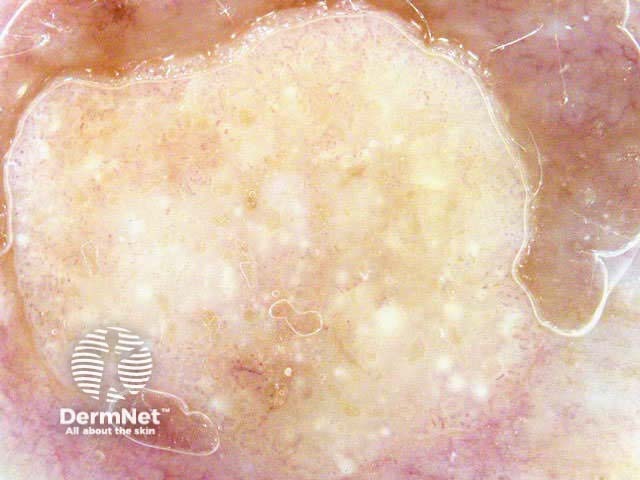
Milia-like cysts are round white or yellow lesions due to intraepidermal keratin. They are characteristically found within a seborrhoeic keratosis. They may also arise within dermal melanocytic naevi, basal cell carcinoma (BCC) and melanoma.



Comedo-like openings are sometimes called ‘crypts’. They are little craters and tend to be dark brown, like irregular globules. They are often associated with fissures (clefts). They are characteristic of seborrhoeic keratoses, but may also be found in dermal naevi. Rarely, they may be found in melanoma.




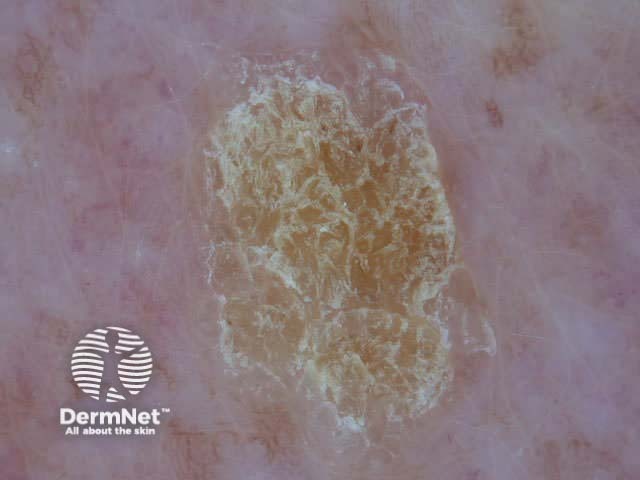
A seborrhoeic keratosis may have a cerebriform or brain-like pattern. The pattern is composed of fissures and ridges mimicking the gyri and sulci of the brain.
This is a useful sign in the absence of comedo-like openings or milia-like cysts.




These are a descriptive term for tan or dark-brown, fine parallel cord-like structures characteristically seen in seborrhoeic keratoses and solar lentigo. Wider cords are called ‘fat fingers’. Fat fingers are also rarely seen in melanoma.



The clinical characteristic of an irregular edge is often seen in melanoma, but is quite common in benign lesions too and is not very useful in the early diagnosis of melanoma dermoscopically.
The border of a skin lesion can fade out (often seen in atypical naevi) or be sharply demarcated in a small segment (typical of melanoma). The sharp cut-off may also occur all the way around in a regular or irregular pattern.
A ‘moth-eaten’ edge is seen as concave areas at the edge of a lesion. This edge is seen in the ephilis and some flat seborrhoeic keratoses and lentigos (benign and malignant).



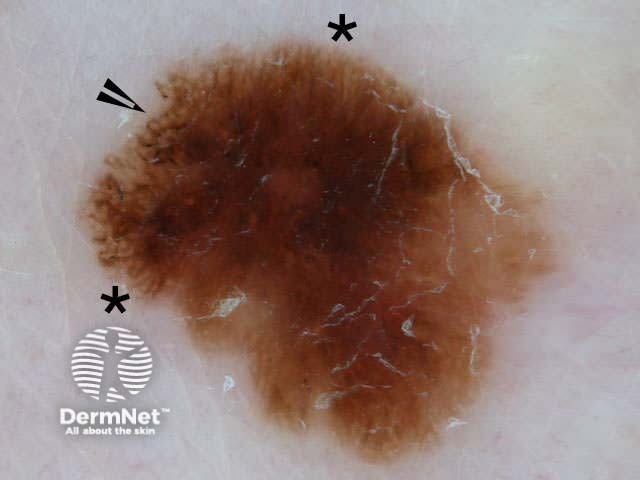
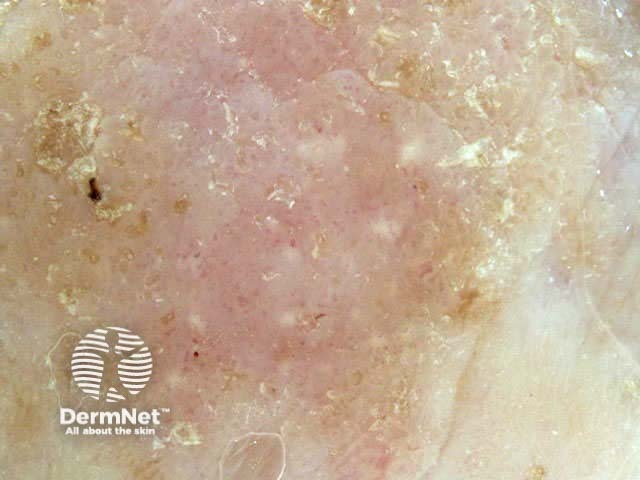
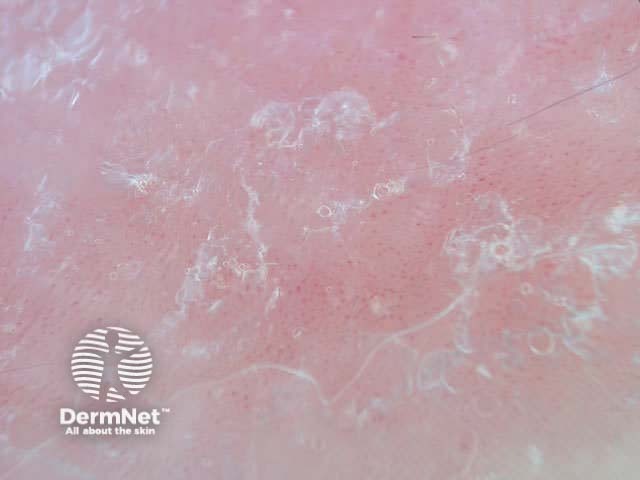
Crystalline structures are shiny, bright white, parallel or orthoganol or disordered linear streaks or short lines. They are seen by contact or non-contact polarised dermoscopy but are not seen on contact non-polarised dermoscopy. They are due to excessive collagen and may be seen in dermatofibroma, scar, basal cell carcinoma with fibroplasia, squamous cell carcinoma, Spitz naevi and melanoma. The earlier term 'chrysalis' structure was a misnomer.




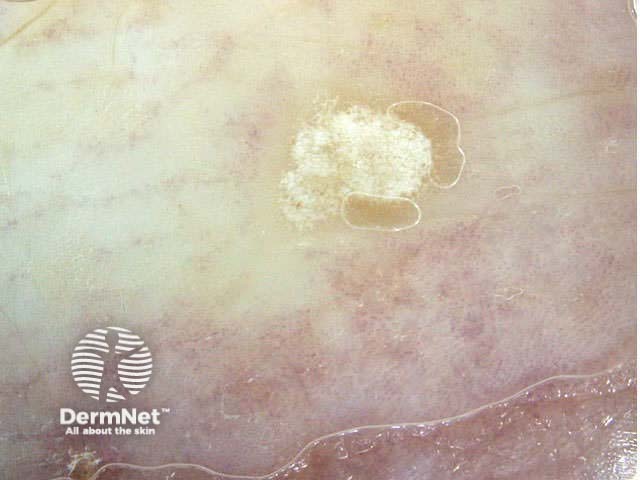
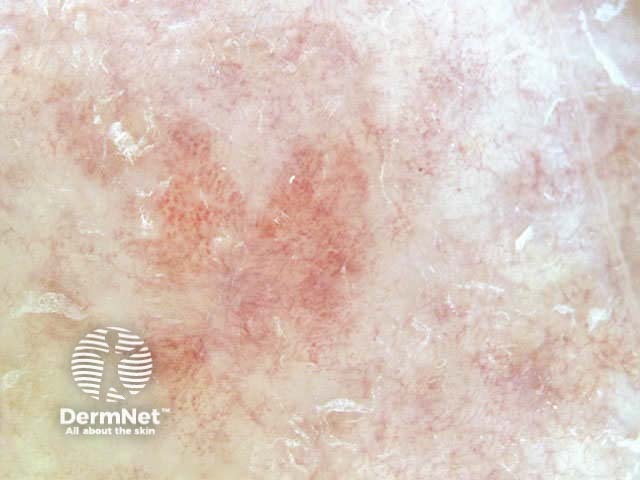
White shiny areas are characterised by similar bright white structures of non-linear shape. Rosettes are four bright white points grouped together like a four-leaved clover, and are typical of actinic keratosis.
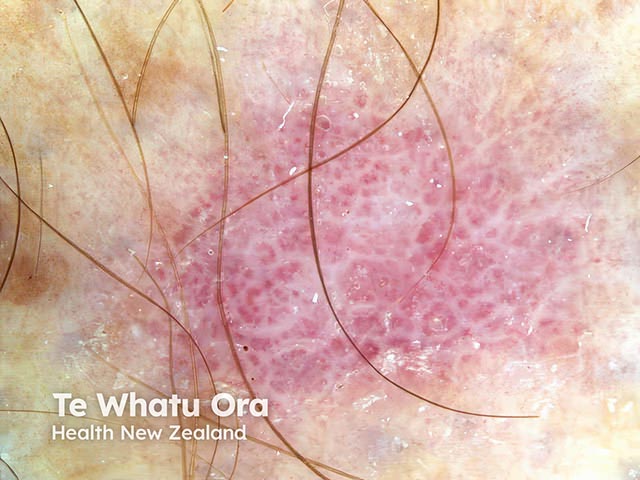
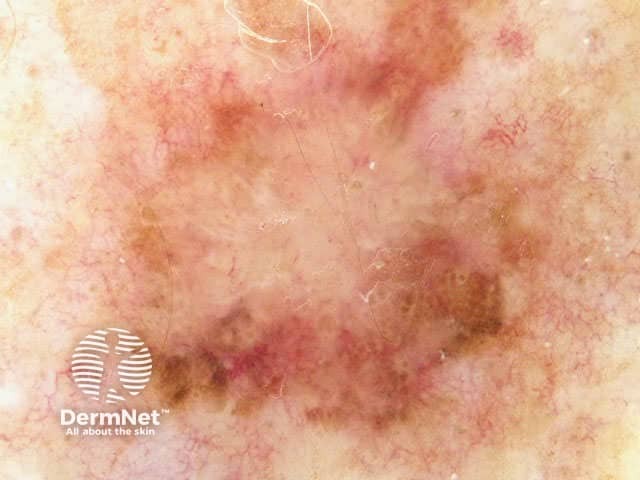
The vascular pattern may be quite distinctive and allow diagnosis of a pink skin lesion, in the absence of pigmentation or dermoscopic structures. If using a contact dermatoscope, take care not to press down on pink lesions, which will exsanguinate the vessels and make diagnosis more difficult.
| Diagnosis | Vascular features |
|---|---|
| Amelanotic melanoma | Dotted or atypical or corkscrew or pink blush or polymorphous vessels |
| Benign melanocytic naevus | Comma shaped vessels |
| Seborrhoeic keratosis | Hairpin vessels, with white halo |
| Basal cell carcinoma | Irregular arborising vessels (thicker lesions) |
| Actinic keratosis | Network of perifollicular vessels |
| Squamous cell carcinoma in situ (Bowen disease) | Focal grouped glomerular vessels |
| Haemangioma | Uniform red, blue or purple lacunes |
| Telangiectasia | Dilated linear and branched vessels |
| Haemorrhage | Red-blue lacunes within a tumour |
| Venous stasis | Diffuse small glomerular vessels |
| Psoriasis | Uniform globular vessels |
| Lichen planus | Very few vessels are seen, or uniform fine linear vessels |








Look at your own moles or those of a family member using dermoscopy. What colours do you see? Evaluate the moles for the following features:
See the DermNet bookstore.

