Introduction
Demographics
Causes
Diagnosis
Clinical features
Prognosis and complications
Treatment
Darier disease is an autosomal dominant genetic disorder classified as a hereditary acantholytic dermatosis. Darier disease typically presents with scaly crusted papules in a seborrhoeic distribution and in skin folds.
Also known as Darier–White disease, Darier disease was previously called ‘keratosis follicularis’, but this is incorrect because the scaly papules do not arise from hair follicles.
The onset of skin changes is usually in adolescence. Darier disease is inherited in an autosomal dominant pattern, which means that a single gene passed from one parent causes the condition. The chance of a child inheriting the abnormal gene if one parent is affected is 1 in 2 (50%) but not all people with the abnormal gene will develop clinical features of the disease.
The abnormal gene in Darier disease has been identified as ATP2A2, found on chromosome 12q23-24.1. This gene codes for the SERCA enzyme or pump (SarcoEndoplasmic Reticulum Calcium-ATPase) that is required to transport calcium within the cell. The exact mechanism by which this abnormal gene causes the disease is still under investigation but it appears that the way in which skin cells join together may be disrupted. The skin cells (keratinocytes) stick together via structures called desmosomes and it seems the desmosomes do not assemble properly if there is insufficient calcium.
Usually, Darier disease is diagnosed by its appearance and family history, but it is often is mistaken for other skin problems.
Diagnosis may require a skin biopsy. The histology is characteristic, known as focal acantholytic dyskeratosis associated with varying degrees of papillomatosis. The pathological features are similar to transient acantholytic dermatosis (Grover disease).
The symptoms and signs of Darier disease vary markedly between individuals. Some have very subtle signs that are asymptomatic and found only on careful inspection. Others have extensive lesions which can cause considerable distress to the affected individual. In an affected person the severity of the disease can fluctuate over time.
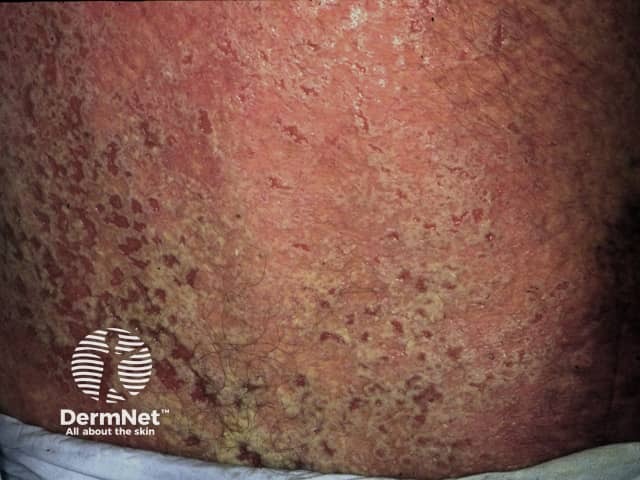
The skin lesions are characterised by persistent, greasy, scaly papules. Affected sites include:
The papules have a firm, harsh feel like coarse sandpaper and may be skin-coloured, yellow-brown, or brown in colour. If several of the small papules grow together they may form larger warty lesions which can become quite smelly within skin folds. There may be a heavily crusted rash similar to seborrhoeic dermatitis.
Other skin signs may include:
Atypical presentations of Darier disease are common.
Acne conglobata (cystic acne) is associated with Darier disease in some individuals.



Warty papules on the dorsum of hands are known as acrokeratosis verruciformis.
A localised variant of Darier disease, in which papules on hands and feet are the main feature is called acrokeratosis verruciformis of Hopf.
Most patients with Darier disease will have longitudinal broad red and/or white stripes in some or all fingernails. A V-shaped nick at the free edge of the nail is very suggestive of Darier disease.



Mucous membranes are the red, moist linings of body surfaces (mouth, oesophagus, rectum, vulva, vagina). Patients with Darier disease may uncommonly have a white cobblestone pattern of small papules affecting the mucous membranes. Overgrowth of the gums may also occur.
Most affected patients develop signs of Darier disease before the age of 20 years.
Flare-ups may be caused by any of the following factors.
In most patients, general health remains good regardless of the severity of the disease. However it can have a major impact on psychosocial functioning and wellbeing (including depression and anxiety).
Treatment of Darier disease is required only if there are troublesome symptoms. Mild disease can be managed with:
Localised Darier disease can be treated by:
Secondary bacterial infection (usually due to Staphylococcus aureus) should be treated with antibiotics. Herpes simplex is treated with aciclovir or valaciclovir.
Severe Darier disease is usually treated with oral retinoids, either acitretin or isotretinoin. Ciclosporin has been reported to be effective in a few patients. There are limited case reports regarding the benefit of dupilumab.



