Introduction - cheilitis
Introduction
Demographics
Clinical features
Differential diagnoses
Diagnosis
Treatment
Cheilitis is the name given to inflamed lips.
Allergic contact cheilitis is allergic contact dermatitis affecting the lip(s). It is due to a type IV hypersensitivity reaction following contact with an allergen and usually presents as an eczema-like inflammation of the outer lip or vermilion margin.


Allergic contact cheilitis is a common cause of lip inflammation and is more common than contact stomatitis, despite considerable overlap in allergen sources. Approximately one quarter of cases of chronic eczematous cheilitis are due to allergic contact. The rest are due to constitutional and irritant factors.
Allergic contact cheilitis is more common in women than men. It can affect all age groups, but adults are more commonly affected than children. However the allergens involved vary in different age groups. These differences reflect the usage patterns of the different age groups and sexes.
Major sources of allergens causing contact cheilitis include:
Common allergen groups that cause contact cheilitis include:
Allergic contact cheilitis usually presents as eczema-like changes on the vermilion margin or skin around the mouth. One or both lips may be red with dryness, scaling and cracking. The changes may be quite localised or affect the whole lip. Involvement of the angles of the mouth may also be seen (angular-cheilitis). The pattern of the reaction may give some clue as to the cause; for example allergy to a musical instrument will develop changes only in that part of the lip in contact with the instrument. Allergic contact cheilitis rarely affects the inner mucosal aspect of the lip.
The patient may report associated itch, burning or pain of the lips.
Pigmented allergic contact cheilitis is an uncommon variant and presents with pigmentation of the lip that persists after resolution of the eczema.
Clinical examination should include, in addition to the lips, the inside of the mouth and general skin. Atopic dermatitis is commonly associated with contact cheilitis.
Contact urticaria of the lip due to a low dose of a frequently used allergen may present as a cheilitis, such as a flavouring in a toothpaste. Foods are a major cause of contact urticaria of the lips.
Oral allergy syndrome should also be considered in people with pollen allergy; onset and recovery are more rapid than with allergic contact cheilitis.
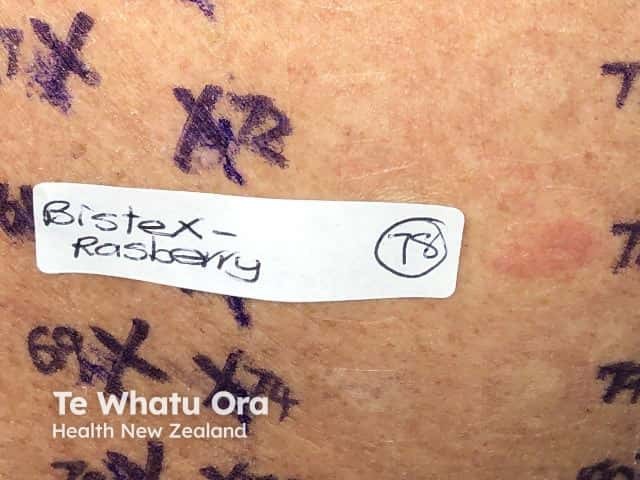
Patch testing is the key to the diagnosis of contact cheilitis. Testing should include the baseline series of patch test allergens as well as cosmetic and toothpaste series, and others suggested by the history. It is most important to also test the patient's own products and musical instruments if possibly relevant. Cosmetics are often applied ‘as is’, but sawdust from wooden instruments should be applied diluted to 10% in petrolatum. A significant number of patients react only to their own products. The relevance of positive results must be assessed, based on careful history taking and clinical examination. Multiple positive reactions are common.

Repeated open application test (ROAT) or start-restart testing may be required for a patient's own products due to irritation under occlusion in patch testing, such as with toothpastes.
Photopatch testing may also be useful when investigating cheilitis when routine patch testing is negative.
Should contact urticaria of the lip be suspected, prick/scratch testing is required.
It is common for patients with allergic contact dermatitis to have a second diagnosis such as atopic cheilitis or irritant contact cheilitis.
Avoidance of the allergen in all of its possible sources is the treatment. The reaction then usually settles quickly.

