Trichilemmal carcinoma typically occurs as solitary exophytic tumour on chronically sun-exposed skin of older individuals.
Histology of trichilemmal carcinoma
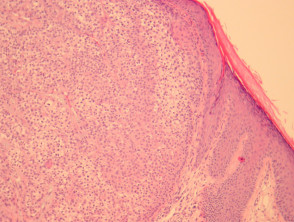
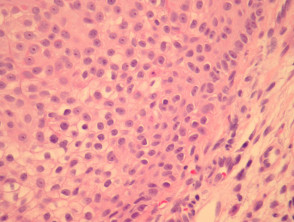
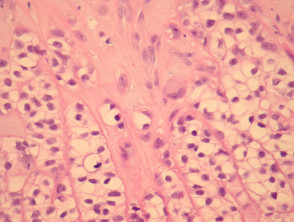
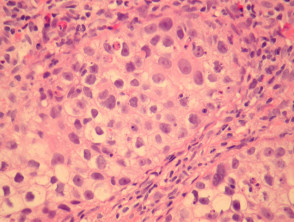
Trichilemmal carcinoma is often well defined laterally and is composed of lobules of atypical keratinocytes exhibiting clear cell change. At the periphery of the lobules the keratinocytes show palisading and are surrounded by a prominent connective tissue sheath (figures 1, 2). The invasive tumour front is usually a broad pushing front. The cells often exhibit marked pleomorphism and numerous mitoses (figure 3, 4).
Trichilemmal carcinoma pathology
Special studies for trichilemmal carcinoma
Immunohistochemical studies are of limited utility. Porocarcinoma or other malignant eccrine/apocrine carcinomas should exhibit some ductal differentiation which can be demonstrated with staining for DPAS or immunostaining for CEA/EMA.
Differential diagnosis of trichilemmal carcinoma
Other clear cell tumours need to be considered:
- Squamous cell carcinoma, clear cell type – SCC lacks peripheral palisading and connective tissue sheath of trichilemmal differentiation (figures 1, 2). SCC typically shows a more infiltrative invasive front.
- Apocrine/eccrine carcinomas – These may sometimes show clear cell differentiation. Identification of ductal differentiation is useful for diagnosing these tumours (see special studies).
- Trichilemmoma – Desmoplastic variants can show an infiltrative growth pattern. Marked pleomorphism and mitoses are absent in benign trichilemmoma.