Introduction
Interstitial granulomatous dermatitis is a rare skin disorder with asymptomatic skin coloured or erythematous lesions with various morphology. Linear cords (“the rope sign”), patches, papules or plaques are reported. Lesions tend to be symmetrically distributed on the trunk and proximal limbs. There is an association with various autoimmune diseases and infections, particularly rheumatoid arthritis.
Histology of interstitial granulomatous dermatitis
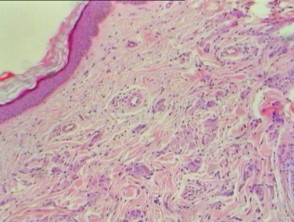
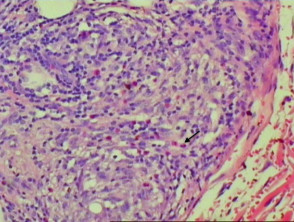
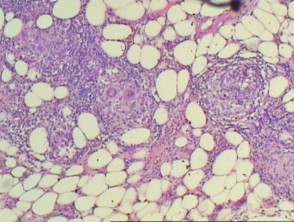
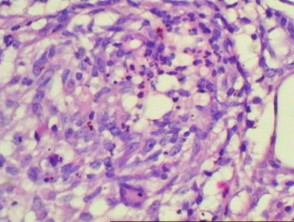
Similar to the clinical heterogeneity of interstitial granulomatous dermatitis, various histological patterns exist. Epidermal changes include scale crust, hyperplasia with perforation and necrosis with epidermal loss. The majority of changes are in the lower dermis with perivascular and interstitial infiltrate with neutrophils, neutrophil dust, lymphocytes and histiocytes (Figure 1). Variable numbers of eosinophils are present (Figure 2, arrow). In some cases, there is palisading of lymphocytes and histiocytes around a focus of neutrophils or collagen fibres. Leukocytoclastic vasculitis and necrobiosis may be present. Inflammation may extend to the subcutis (Figures 3, 4). Fibrosis may be seen in later stages.
Interstitial granulomatous dermatitis pathology
Special studies of interstitial granulomatous dermatitis
Immunofluorescence may be positive for IgM, C3 and fibrinogen in dermal blood vessels.
Differential diagnosis of interstitial granulomatous dermatitis
Leucocytoclastic vasculitis: Neutrophils and dust in interstitial granulomatous dermatitis are more widely distributed throughout the dermis in addition to around vessels.
Granuloma annulare: Changes may be similar, particularly to the interstitial variant of granuloma annulare. Mucin deposition is a more prominent feature in granuloma annulare.
Necrobiosis lipoidica: Giant cells are more commonly seen in necrobiosis lipoidica. The presence of eosinophils and neutrophils (and dust) favours interstitial granulomatous dermatitis.