Created 2009.
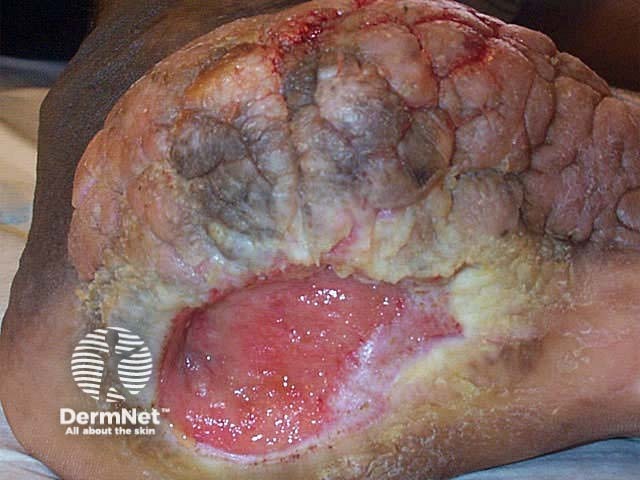
Impaired wound healing may be attributed to defects in the normal tissue response to injury and to poor treatment of the wound. Chronic wounds are defined as those that do not appear to follow the normal healing process in less than 4 weeks. These wounds are most commonly located on the lower leg, foot, and pelvic region. Healing is more difficult because the aetiology of the wound is harder to determine, and the measures to reverse the medical abnormalities are often complex.
Knowledge about the science of wound healing is expanding. In the near future we can anticipate new therapies for slow or abnormally healing wounds that will be based on genetics and immunology. More effective biological dressings and growth factors are already available and are proving useful for selective patients.
Hypertrophic scars and keloids are thickened scars due to excessive synthesis of collagen after an acute injury. The terms overlap, but in general hypertrophic scars develop within the boundary of the original wound and regress in time whereas keloids extend beyond the wound boundary and tend to remain elevated. Hypertrophic scars follow known injury such as surgery, laceration, abrasion or deep inflammatory skin disease such as acne. They are more likely if there is excessive tension on the wound, tissue infection or electrosurgery. Keloids may also arise spontaneously and sometimes continue to slowly grow for many years.
Hypertrophic scars and keloids most frequently arise in young adults and are particularly prevalent in black-skinned individuals. They are equally common in males and females. Although often asymptomatic, these scars may also be pruritic and/or tender. They are firm or hard, skin-coloured to bright red, smooth, elevated nodules. Keloids may have claw-like extensions far beyond the original wound. They are particularly frequently seen on earlobes, shoulders, upper back and anterior chest.
The histology of a hypertrophic scar is whorled fibrous tissue with haphazardly arranged fibroblasts. Keloids have similar features with thick eosinophilic bands of collagen.
Management is challenging. Susceptible individuals should avoid cosmetic procedures such as excision of benign naevi and body piercing. Any surgical procedure should be undertaken with careful attention to optimum conditions for healing.
Active treatment of hypertrophic and keloid scars attempts to reduce collagen formation and actively destroy it by inducing collagenase. Treatment may include:


Many intrinsic and extrinsic factors can impair wound healing.
Local factors
Regional factors

Systemic factors
Miscellaneous factors
Smoking
The association between poor surgical outcome and smoking has been recognised for a long time. Smoking increases the risk of wound infection, graft or flap failure, tissue necrosis and haematoma formation. The pathogenesis is unclear but involves:
Aging
There are age and sun-induced changes in the structure and function of the skin resulting in thinner, less elastic tissue that bruises easily. However, these changes have little impact on acute wound healing. Chronic wounds are prevalent in the elderly but poor healing is related to co-morbid conditions rather than age alone. Ageing results in dysfunctional molecular mechanisms that affect the ability to repair damaged cells and tissues. This may lead to neoplastic transformation of a normal cell into one with unlimited growth potential i.e. skin cancer. Neoplasia prevents normal healing processes; ulceration is characteristic for basal and squamous cell carcinomas.


Inadequate nutrition
Carbohydrates, protein and amino acids, fatty acids, minerals and vitamins are required for normal wound healing. Abnormal nutritional states may arise because of:
Delayed wound healing occurs in patients with hypovitaminosis A (retinol). In contrast, excessive granulation tissue may arise in hypervitaminosis A or in patients treated with synthetic retinoids (isotretinoin or acitretin).
Scurvy is due to deficiency of vitamin C (ascorbic acid). Cutaneous features include poor wound healing, follicular hyperkeratosis, ‘corkscrew’ hairs, petechiae and ecchymoses.
Essential fatty acid deficiency has been most often described in patients on total parenteral nutrition prior to routine addition of fat supplementation. In the skin, lack of essential fatty acids results in scaling, erythema and poor wound healing. This can be corrected by topical or oral linoleic acid (found in oil of evening primrose, safflower or sunflower seed).
Severe zinc deficiency arises in the rare inherited disorder acrodermatitis enteropathica and in patients on total parenteral nutrition without zinc supplementation. Less severe zinc deficiency is associated with diets consisting mainly of grains and refined foods, old age, pregnancy, lactation and alcoholism. It may also arise in sickle cell anaemia or if there is hyperzincuria due to liver or kidney disease. In these disorders, zinc supplementation may help wound healing.
Obesity is associated with poor wound healing because of infection, oedema and increased prevalence of diabetes.
Diabetes mellitus
Diabetes gives rise to high risk of major complications in wounds, including infection and amputation. Vascular, neuropathic, immune function, and biochemical abnormalities each contribute to delayed healing. Even careful wound care in a patient with excellent glucose control may fail. Chronic infection itself contributes to raised blood glucose levels.

Immune deficiencies
These may be due to aging, disease or drugs and may result in delayed wound healing because of intrinsic defects and secondary infection.
Coagulation and haematological defects
Excessive bleeding and abnormal clot formation prevent normal healing.

Abnormal collagen
There are at least six subtypes of Ehler Danlos syndrome, which involve genetic defects in collagen and connective tissue synthesis and structure. They are characterised by varying degrees of fragile and atrophic or ‘cigarette paper’ scars.


Infection of intact skin may create a wound de novo, but more often bacterial invasion follows removal of at least the stratum corneum. About 2-3% surgical wounds are complicated by infection; the risk of infection is greatest during the first 48 to 72 hours. It is more likely in patients with impaired haemostasis or inflammation such as those with advancing age, diabetes, steroid therapy and other immunosuppressants, obesity, severe malnutrition, compromised circulation, and infection in other sites.
Tissue levels of greater than 105 pathogenic organisms are correlated with clinical infection i.e. erythema, oedema, pain, purulence and lymphadenitis. Systemic signs of infection include fever, tachycardia, hypotension, delirium, and alterations in mental status in older patients.
Histological features of infection include invasion of viable tissue by pathogens and polymorphonuclear (PMN) leukocyte response, although PMNs are also a feature of wound healing per se.
Surgical or acute wound infection is most frequently due to Staphylococcus aureus and sometimes Streptococcus pyogenes and aerobic gram-negative bacilli. Enteric Gram-negative rods, Group D enterococcus and Bacteroides fragilis group affect wounds relating to the gut flora, while Streptococcus spp., pigmented Prevotella and Porphyromonas spp. and Fusobacterium spp. may be recovered in wounds proximal to the oral area.



Chronic wounds may be colonised by multiple species of aerobic and anaerobic bacteria but are at lower risk of infection. Colonisation may be of benefit to granulation and epithelization but it may also impair wound healing. Aerobic bacteria are isolated from most chronic wounds, particularly coagulase-negative Staphylococcus, S aureus, ß-haemolytic streptococci, Str. viridans, Corynebacterium species, E coli, K pneumoniae, and Enterobacter aerogenes. Cutibacterium acnes and Bacteroides genus are the most prevalent anaerobic isolates.


Infection may sometimes result in a proliferative response i.e. excessive granulation tissue as arises in pyogenic granuloma and ingrown toenails.



Prevention of wound infections
Surgical wounds require careful antiseptic technique in patient preparation, during surgery and in postoperative patient care. For most procedures prophylactic antibiotics are unnecessary and risk adverse drug reactions. However they should be considered in those at high risk of wound infection especially if there are multiple predisposing factors.
Where possible, correct for intrinsic patient risk factors:
Treatment of wound infection
An infected wound must be cleansed and debrided to remove necrotic tissue and foreign bodies. Techniques include:
Treatment with topical antibiotics is popular but undesirable because of increasing rates of bacterial resistance. Current interest is focused on antimicrobial moisture-retentive dressings, honey, essential oils and cationic peptides.
More serious local and systemic infections should be treated with systemic antibiotics: penicillins, cephalosporins, aminoglycosides, fluoroquinolines, and sulfonamides are most often prescribed. Other antibiotics include clindamycin, metronidazole, and trimethoprim.
Other measures to improve tissue oxygenation are also important, such as minimising oedema by elevation and compression.
The wound healing process can be involved in the pathogenesis of skin disease. The isomorphic response or Koebner phenomenon occurs in psoriasis, lichen planus, vitiligo, sarcoidosis and other conditions. The skin disorder appears in an area subjected to minor trauma or a scar, resulting in characteristic shapes eg linear plaques. This term may also be used to describe a linear pattern of infection in traumatised skin e.g. viral warts.
Skin cancer (basal or squamous cell carcinomas) may be precipitated by injury and arise in chronic injury such as from X-radiation, thermal burns, venous ulceration.
Pathergy is the development of a sterile pustule due to minor trauma e.g. venepuncture, frequently followed by ulceration. It is a characteristic feature of pyoderma gangrenosum and Behcet syndrome.






Find evidence that various measures to reduce scarring are effective,
Information for patients
See the DermNet bookstore

