Introduction
Adenoid cystic carcinoma typically arises within salivary glands. Primary cutaneous adenoid cystic carcinomaand adenoid cystic carcinoma of the breast are rare but well recognized.
Histology of adenoid cystic carcinoma
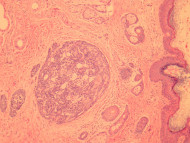
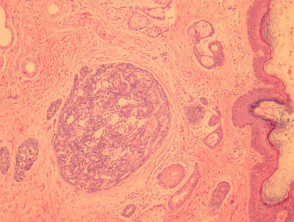
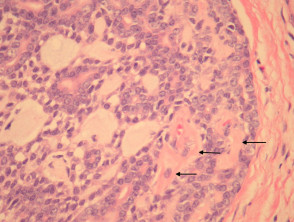
In primary cutaneous adenoid cystic carcinoma, the tumour involves the dermis and may invade the subcutis (figure 1). The tumour is composed of basaloid cells arranged in a ductal or cribriform pattern. Characteristically there are eosinophilic hyaline membranes lining the pseudolumina within the tumour (figure 2, arrows).
Adenoid cystic carcinoma pathology
Special studies of adenoid cystic carcinoma
Adenoid cystic carcinoma is typically a morphologic diagnosis. The basement membrane material may be highlighted with PAS stain.
Differential diagnosis of adenoid cystic carcinoma
Cylindroma — These tumours exhibit a typical “jigsaw puzzle” architecture rather than the irregular cribriform and tubular architecture of adenoid cystic carcinoma.
Basaloid squamous cell carcinoma – Can mimic adenoid cystic carcinoma. p63 immunohistochemistry can be helpful if this is a diagnostic consideration. Diffuse p63 positivity is more commonly seen with SCC.