Introduction
Histology
Special stains
Variants of basal cell carcinoma
Differential diagnosis
Basal cell carcinoma (BCC) is the most common form of nonmelanoma skin cancer occurring in the skin. It is a locally destructive tumour with varied clinical and histological appearances.
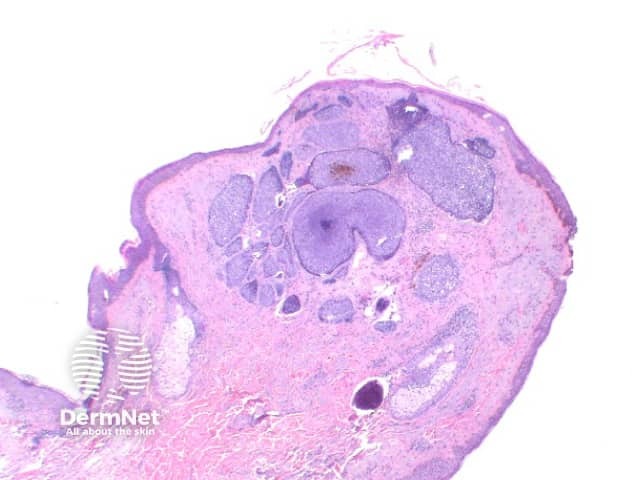
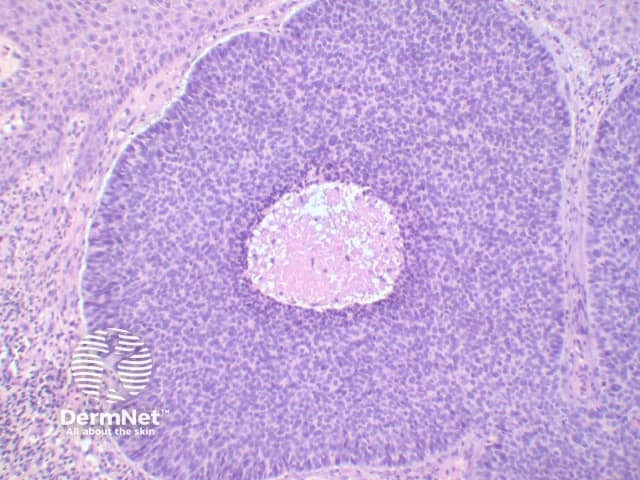
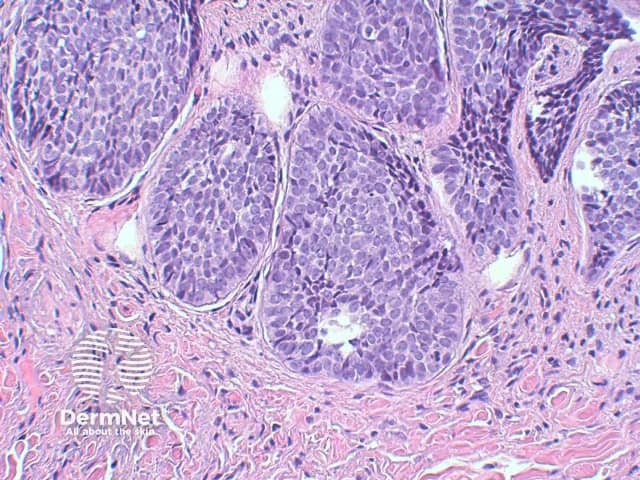
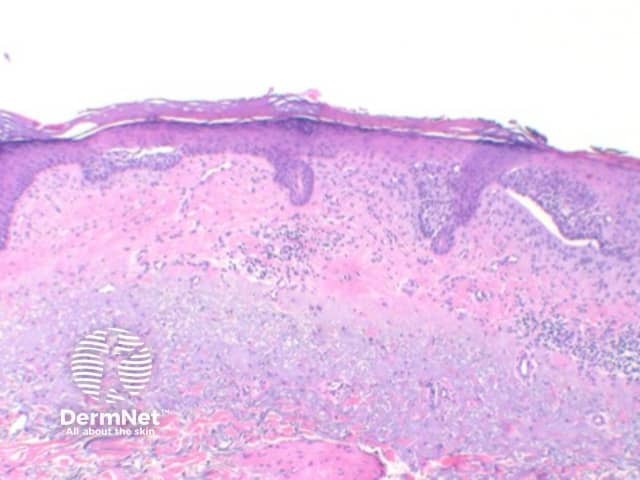
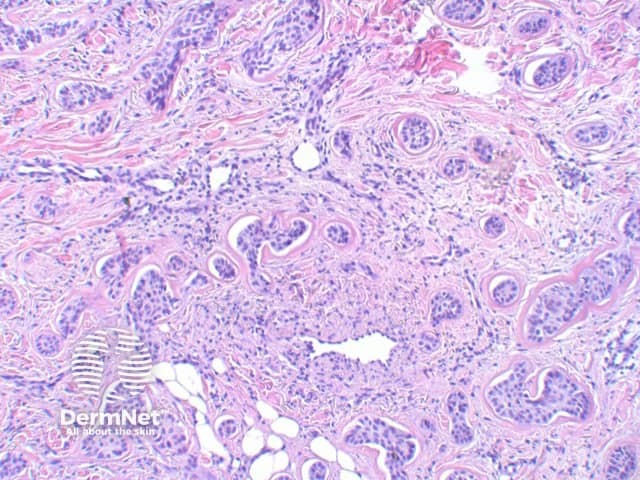
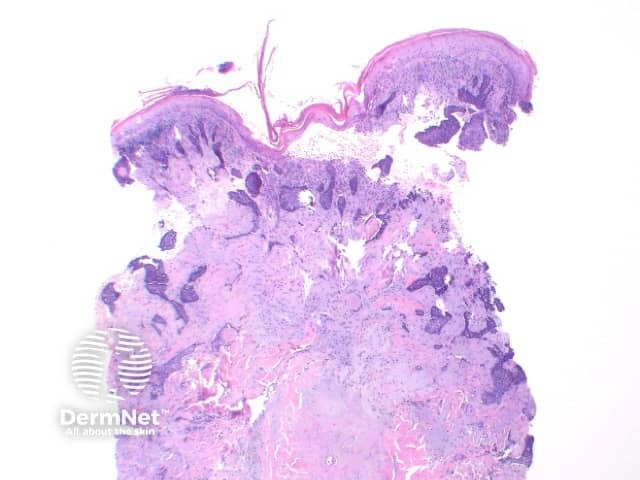
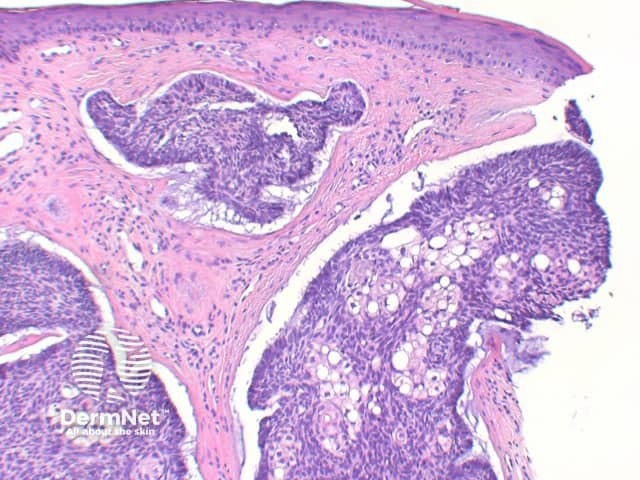
The key feature of basal cell carcinoma at low power magnification is of a basaloid epithelial tumour arising from the epidermis (figure 1). The basaloid epithelium typically forms a palisade with a cleft forming from the adjacent tumour stroma (figure 2). Centrally the nuclei become crowded with scattered mitotic figures and necrotic bodies evident (figure 3). A useful distinguishing feature from other basaloid cutaneous tumours is the presence of a mucinous stroma (figure 4). Some tumours may also show foci of regression, seen as areas of eosinophilic stroma with lack of basaloid nests.
Basal cell carcinoma stains positively with cytokeratin, though favouring cytokeratins from the follicular epithelium. BerEP4 is diffusely present in most tumours, while EMA is infrequently positive.
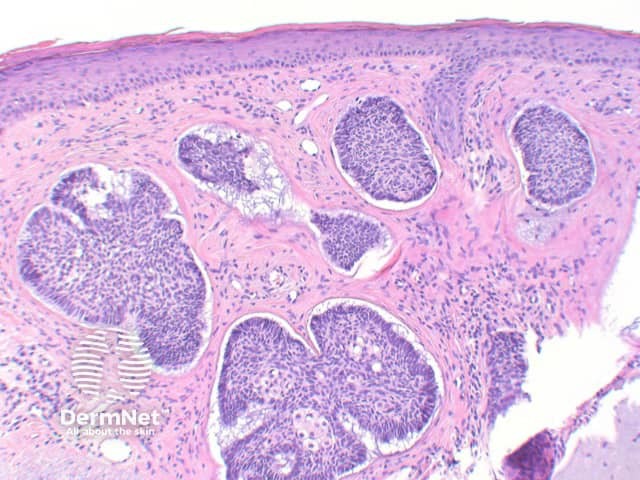
Superficial BCC: This variant show multifocal nests of atypical basaloid epithelium arising as buds from the basal layer of the epidermis. These nests remain confined to the papillary dermis (Figure 5)
Nodular BCC: The tumour forms a solid tumour nodule or nodules which may extend into subcutaneous tissues. Cartilaginous invasion is unusual (figure 1).
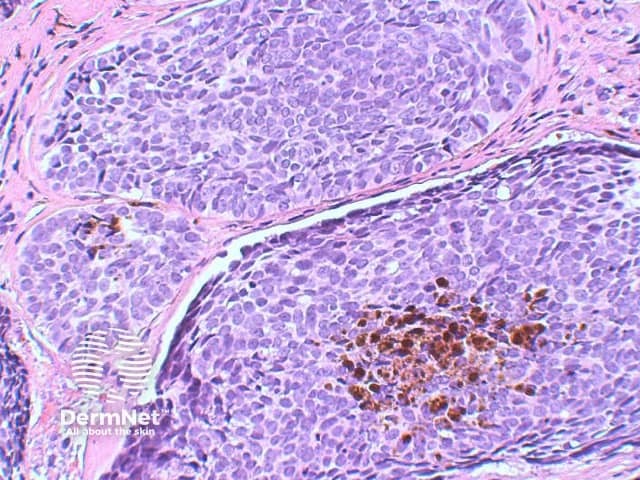
Pigmented BCC: Focal deposits of melanin are evident throughout the tumour. An increased number of melanocytes may also be seen within the tumour, and scattered melanophages may be present in the surrounding stroma (figure 6).
Micronodular BCC: While commonly forming a nodular architecture, the tumour is comprised of multiple small nests. This tumour may also exhibit extensive infiltration into surrounding tissue, and is included within the poorer prognosis subtypes of tumour given the increased risk of local recurrence (figures 7,8,9).
Basosquamous carcinoma: While this tumour may also be considered in the differential diagnosis as within the umbrella of squamous cell carcinoma, the clinical and histological features more closely resemble basal cell carcinoma. The cellular morphology shows areas of large, pale squamoid cells, but lack keratinisation. This therefore shows close resemblance to the metatypical type. These tumours will stain positively with BerEP4 while usually negative for EMA.
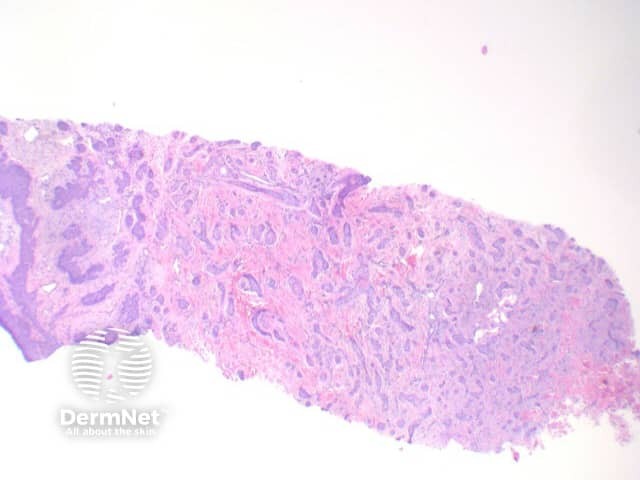
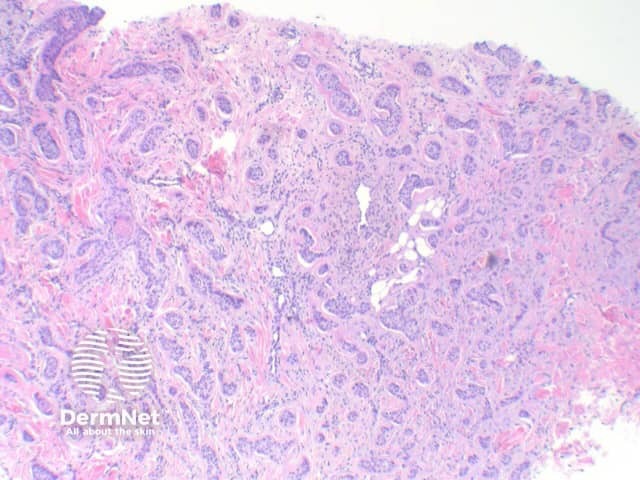
Infiltrating BCC: In this aggressive subtype, the tumour shows extensive infiltrating strands and cords of atypical basaloid epithelium (figures 10,11).

Metatypical BCC: Now rare subtype, demonstrating progression of typical basal cell carcinoma into areas with large pale cells. Peripheral palisading and clefting is lost.
Infundibulocystic BCC: This variant shows multiple small cysts containing cornified material with differentiation towards the infundibulum. In distinguishing from trichoepitholioma, it lacks papillary mesenchymal bodies, but frequently retains a mucinous stroma.
Sclerosing BCC: The tumour shows strands of atypical basaloid epithelium set in a densely fibrotic stroma.
Sebaceous differentiation: Basal cell carcinoma can also occasionally show areas of significant sebaceous differentiation (figure 12). This needs to be differentiated from sebaceoma, as discussed below.
Trichoepithelioma: The epithelium of trichoepithelioma demonstrates intimate integration with the surrounding matrix which is often cellular and fibromyxoid and show stroma. In contrast, basal cell carcinoma typically exhibits at least some retraction (clefting) between the epithelial cells and the surrounding epithelium and may show mucin deposition. Papillary mesenchymal bodies can serve as an important clue to trichoepithelioma. Immunohistochemistry is typically unhelpful but numerous stains are sited in the literature including Bcl-2, Ber-Ep4 and CD34. BCL2 staining is diffusely positive in basal cell carcinoma, while highlighting the basal layer of trichoepitheliomas. CD10, while positive in basal cell carcinomas and trichoepithelioma, tends to show peritumoral stromal reaction also.
Sebaceoma: This tumour will usually show a more lobulated architecture, and lack palisading, clefting and mucinous stromas. Immunostaining may be helpful with sebaceoma rarely positive for BerEP4, while typically positive with EMA.
Microcystic adnexal carcinoma: This can be difficult to distinguish from infiltrating basal cell carcinoma and desmoplastic trichoepithlioma. Deep invasion, extensive perineural invasion and convincing ductal (glandular differentiation) may favour microcystic adnexal carcinoma. Immunohistochemical studies with CK20 can be extremely useful. Isolated native Merkel cells stain with CK20 in desmoplastic trichoepithelioma but will be absent in microcystic adnexal carcinoma.

