Introduction
Perforating folliculitis presents with multiple follicular papules on the extremities and buttocks. Numerous disease associations have been described. It is well described to cause an itchy eruption in chronic renal failure patients on dialysis.
Histology of perforating folliculitis
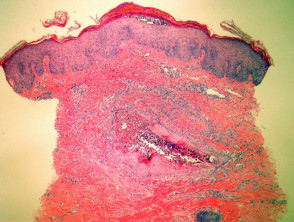
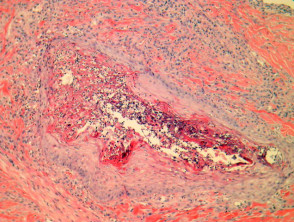
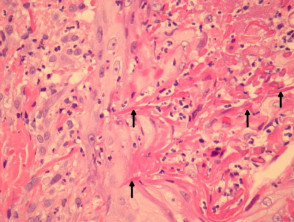
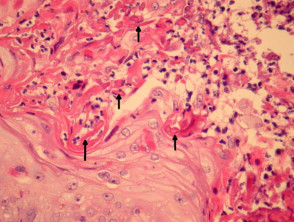
Sections show a suppurative folliculitis on low power examination (figure 1). Higher power examination shows debris and acute inflammation within a distorted follicle (figures 2-4). Collagen fibres and elastic fibres can be seen penetrating into the follicular space (figures 3-4, arrows highlight extruded fibres). There is frequently degeneration of dermal connective tissue adjacent to the involved follicle.
Perforating folliculitis pathology
Special studies for perforating folliculitis
The extruded fibres can be demonstrated with an elastic stain (e.g. EVG) and collagen stain (e.g. trichrome)
Differential diagnosis of perforating folliculitis
Elastosis perforans serpiginosa (EPS) – The clinical features can be helpful in providing an accurate distinction. Elastic fibres are not increased in perforating folliculitis but are increased and abnormal in EPS. Perforation of collagen as well as elastic fibres should not be seen in EPS
Reactive perforating collagenosis – There may be some pathogenic overlap with this entity. Both entities share similar clinical features in chronic renal failure patients.
Kyrle disease – Some authorities regard this as a perforating folliculitis.