Introduction Causes Psychological effects Clinical features Treatment Further research
Hair loss (alopecia) is a common problem that affects up to 50% of men and women throughout their lives [1].
Hair loss can be broadly categorised into scarring (cicatricial) alopecia and non-scarring (non-cicatricial) alopecia, with hair loss on the scalp further classified as focal or diffuse alopecia.
Hair loss can occur anywhere on the body, but most commonly affects the scalp. Abundant scalp hair has societal and cultural importance. Loss of scalp hair, eyebrows, and eyelashes frequently leads to psychological distress.

The main causes of hair loss depend on whether the type of hair loss is scarring or non-scarring, and focal or diffuse.
Scarring alopecia is rare and is caused by injury, infection, and inflammatory skin disorders such as discoid lupus erythematosus, lichen planopilaris, and folliculitis decalvans.
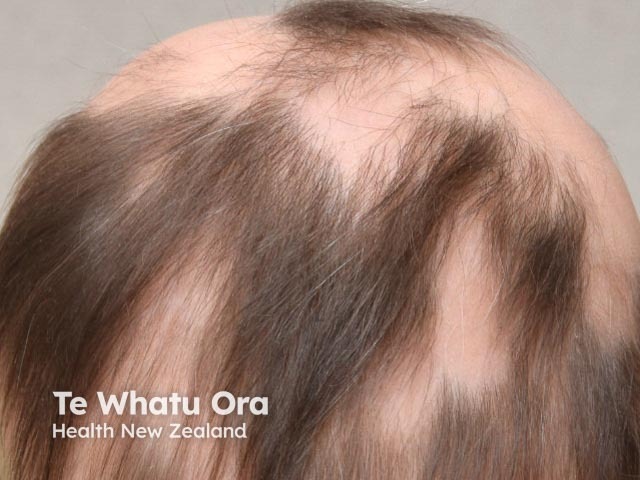
Non-scarring focal alopecia is usually caused by tinea capitis, a fungal skin infection, or alopecia areata (an autoimmune disorder).
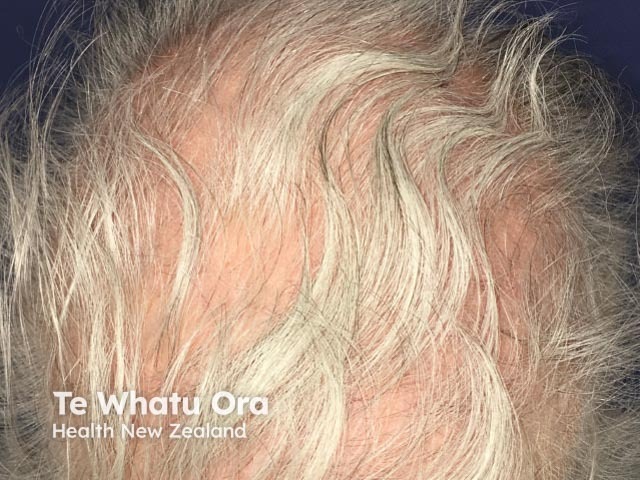
Diffuse hair loss may follow hair shedding, which is usually stress-induced hair loss (telogen effluvium) or is due to genetically determined male or female pattern hair loss [2]. Diffuse hair loss can also be caused by alopecia areata, medications, and various systemic illnesses including anaemia, hyperandrogenism, and thyroid disease.
Psychiatric disturbances, such as acute anxiety and endogenous depression, have also been considered possible causes of diffuse hair shedding [3].
Whatever the cause, the more hair is lost, the lower the likelihood of regrowth.
Research into the psychological problems associated with hair loss is limited.
The evidence confirms that the experience of hair loss is psychologically damaging, causing intense emotional suffering, and often leading to personal, social, and work-related problems. People with severe hair loss are more likely to experience psychological distress than those with mild hair loss [4]. The loss of hair changes a person’s looks, particularly when the eyelashes and eyebrows are affected as they define a person's face. Hair loss may be seen as a failure to conform to the norms of physical appearance within society [4].
The relationship between hair loss and psychosocial consequences may be complicated by hair loss that eventuates from a stressful experience or life event, which then leads to further distress, anxiety, and depression [5]. Women who experience high levels of stress are 11 times more likely to experience hair loss than those who do not report high stress levels [6].
Compared with the general population, people with hair loss have an increased prevalence of psychiatric disorders, including a major depressive episode, an anxiety disorder, social phobia, or a paranoid disorder [7].
Hair loss may lead to depression, anxiety, and social phobia.
These symptoms can have a severe impact on an individual’s mental health, ability to work or study, and well-being.
Anxiety and depression caused by hair loss can be treated using cognitive behavioural therapy and support groups, as well as by medication such as antidepressants [9].
Psychological treatment is important for people with hair loss, but the best method is not certain and will differ from patient to patient. Research has predominantly been focused on the general issues of coping with hair loss rather than on specific psychological treatment strategies.
A strong theoretical understanding of the psychological impact of alopecia is required, including knowledge of the immune system, the stress response, and psychological responses to hair loss. Appropriate treatment strategies and regimes need to be established, implemented, and studied in a clinical setting.
Self-consciousness about body image is consistently portrayed and commented upon in the media. The role of the media in emphasising an expectation of a full head of hair should be explored, as well as how it can be used to educate society about hair loss and tolerance of people’s physical differences.

