Structure of a normal hair follicle
Introduction
Causes
Bubble hair
Beaded hair/monilethrix
Pili torti
Bamboo hair / trichorrhexis invaginata
Trichorrhexis nodosa
Trichothiodystrophy
Acquired progressive kinking of hair
Loose anagen hair syndrome
Ringed hair/pili annulati
Pili bifurcati
Spun glass hair/pili trianguli et canaliculi
Woolly hair
Tufted hair/pili multigemini
Treatment
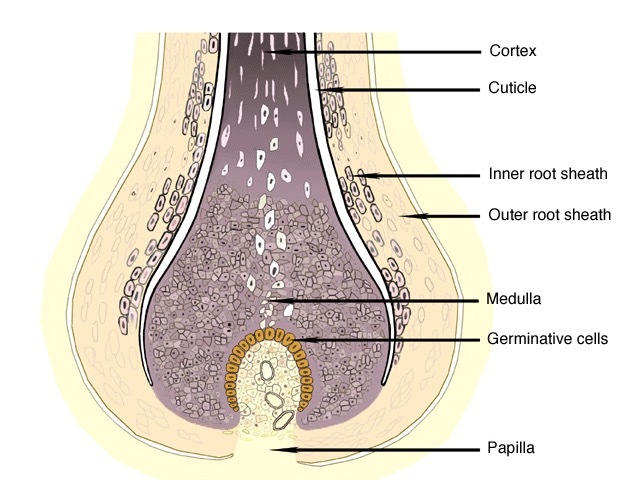
The hair follicle is the structure of skin from which the hair shaft emerges. The hair shaft grows from germinative cells in the hair bulb deep within the dermis.
The follicle is lined by inner and outer sheaths, which protect and shape the growing hair.
A muscle called the arrector pili attaches to the outer root sheath below the sebaceous gland. When the erector pili muscle contracts, e.g. when cold, the hair shaft stands up (goosebumps).
A single hair shaft is made up of three parts:
The medulla and cortex have pigment cells responsible for hair colour.
The cuticle is the outer and strongest part of the hair shaft. It is made up of dead flattened cells that overlap each other. The cuticle is keratinised i.e., the cells are largely made of a protein called keratin; keratin is also an important component of skin and nails.
The sebaceous gland produces sebum, which protects the hair shaft and acts as a natural conditioner.
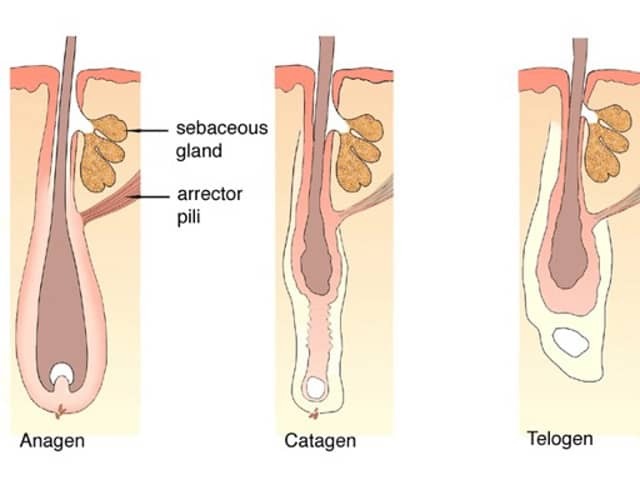
Hair grows in cycles so the structure of an individual hair apparatus varies.
Then the new anagen hair shaft starts to germinate within the same follicle, and it pushes out the telogen hair resulting in normal hair shedding or moulting.
A hair shaft defect is any structural abnormality of the hair shaft. Some hair shaft defects are easily diagnosed with the naked eye, others may require microscopic examination (trichoscopy).
Hair shaft defects may result in:


Hair shaft defects may be due to external injury or genetic abnormality.
Repeated physical injury is the commonest cause of increased hair fragility. This may be due to:
A chemical injury may be caused by:


Genetic hair shaft abnormalities may be broadly divided into two types: those with increased hair fragility and those without increased hair fragility.
Increased fragility |
No increased hair fragility |
|---|---|
Bubble hair is characterised by hair shafts with large “bubbles” within them. These thin the hair cortex and break the hair shaft.
There may be a genetic predisposition to bubble hair. However, the presentation is often precipitated by an external injury such as use of a hairdryer, physical or chemical hair straightening or curling irons.
The name beaded hair reflects hair shafts with narrowed segments between “nodes” of normal thickness. It is also called monilethrix. The scalp is most commonly involved.
The affected hair shafts appear beaded a few months after birth. They break off leaving patches of the scalp with abnormally short hairs. The scalp may also have a rough appearance because of a build-up of keratin around the hair follicle.
Monilethrix is inherited as an autosomal dominant characteristic. This means an affected individual has a 50% chance of passing it on to each of their male and female children. It is caused by changes in the keratin gene cluster at chromosome 12 (gene map locus 12q13, OMIM ID #158000). Recent studies suggest mutations of the keratin genes KRT31, 86 and 81.
There is no known treatment.


Pili torti describes a flattened hair shaft with clusters of narrow twists at irregular intervals. The hairs are abnormally fragile. It may be genetic in origin (inherited) or acquired.
When inherited, pili torti may be present at birth or appear during infancy (OMIM ID %261900).
Pili torti is associated with a number of inherited syndromes.
Acquired pili torti may arise in the following circumstances:
Bamboo hair or trichorrhexis invaginata is due to abnormal keratinisation. The hair shaft cortex is structurally weak at specific points along its length. Harder adjacent segments of the hair shaft impact into these softer portions creating a ball and socket appearance. The hair shaft may break with minimal trauma.
The cause is a mutation in the SPINK5 gene (locus 5q32, OMIM ID *605010)
Trichorrhexis invaginata is a classical feature of Netherton syndrome (OMIM ID #256500).
Trichorrhexis nodosa is the most common abnormality of the hair structure. When a weak hair shaft partially fractures and the cortical cells fragment, uneven spurs form at the fracture point.
Trichorrhexis nodosa may be congenital and occurs in children with intellectual disability and argininosuccinic aciduria.
Trichorrhexis nodosa may also be acquired, due to hair straightening, overheating by a hairdryer, frequent swimming in chlorinated water, excessive traction with tight braids and other forms of hair trauma.
There have been case reports of trichorrhexis nodosa improvement with low-dose oral minoxidil treatment.

In trichothiodystrophy, the hair shafts are deficient in sulphur resulting in transverse fractures. Polarising microscopy reveals intermittent dark bands.
Trichothiodystrophy may occur as an isolated hair shaft abnormality or may be associated with photosensitivity, ichthyosis, brittle hair, intellectual disability, short stature, neurologic abnormalities, and nail and teeth dystrophy (Tay syndrome, OMIM ID %275550).
Acquired progressive kinking of hair is also called pubeshaarnaevus because it resembles pubic hair. In this rare disorder, scalp hair becomes progressively curly, frizzy, dry and difficult to comb.
It usually affects the vertex or frontotemporal area of young men and may progress to male pattern balding (androgenetic alopecia).
Acquired progressive kinking of hair may also be a side effect of retinoid therapy.
Loose anagen syndrome is due to defective keratinisation of the inner root sheath, rather than the hair shaft itself. The loose hair shaft can be easily pulled out of the follicle, leaving localised or diffuse bald areas of the scalp.
On light microscopy, the abnormal hairs are seen to be in the anagen phase and often appear twisted with longitudinal grooves and ruffled cuticles.
Loose anagen (hair) syndrome results in short, brittle hair. Although both sexes may be affected, it most often presents in young girls over the age of 2 years. They usually have blond or red coloured hair.
It may be diagnosed by the painless extraction of at least 10 hairs on a hair pull test of which over 80% of the hairs are in the anagen phase.
It is inherited as an autosomal dominant condition with variable penetrance (OMIM ID 600628). There is no known treatment.






Pili annulati or ringed hair is used to describe hair in which there are scattered groups of air-filled 'bubbles' along the hair shaft. These appear as bright bands when seen with reflected light (OMIM ID %180600).
Pili bifurcati describes abnormal branching of the hair shaft. This can occur at multiple points. The branches often fuse together again further up the shaft. Each branch has its own cuticle.
Spun glass hair is also called pili trianguli et canaliculi, uncombable hair syndrome and cheveux incoiffables. The hair shafts have an irregular, triangular shape on cross-section and an abnormal longitudinal groove running along the shaft.
Spun glass hair is due to abnormal keratinisation of the inner root sheath. This forms an inflexible tube through which the hair shaft must pass, distorting its shape and rendering it stiff and brittle. Light reflected from the flattened surface gives the hair a “spun glass” appearance.
Spun glass hair is associated with atopy (eczema), alopecia areata and ichthyosis vulgaris. (OMIM ID #191480).
There is no known treatment for spun glass hair. However, the condition may improve with age.

Woolly hair describes unusually frizzy, tightly coiled hair. The hair shafts have elliptical cross-sections, axial twisting and scattered areas of splaying.
It may affect the entire scalp or just a small area when it is considered a type of birthmark (naevus), the woolly hair naevus.
Woolly hair may be inherited as an isolated condition (OMIM ID #194300) or present as part of a syndrome.
Other conditions that may be associated with the presence of woolly hair include keratosis pilaris, ichthyosis, abnormal teeth and nail dystrophies.



Tufted hair or pili multigemini describes multiple hair shafts bunched together and emerging from one follicle (like a toothbrush or doll's hair). Light microscopy confirms that all the hairs are surrounded by a single outer root sheath. The hair shafts are normal.
Tufted hair is a feature of scarring inflammatory scalp conditions, particularly the severe forms of scalp folliculitis known as folliculitis decalvans and dissecting cellulitis.



At present, there is no specific treatment for inherited structural hair disorders. Occasionally there is a spontaneous improvement as the child ages.
In acquired structural hair disorders, stopping exposure to the causative agent may lead to improvement.
Gentle hair care is recommended. Short hairstyles are advisable. In some cases, a wig or hairpiece may be the most practical approach.

