Introduction
Demographics
Causes
Clinical features
Complications
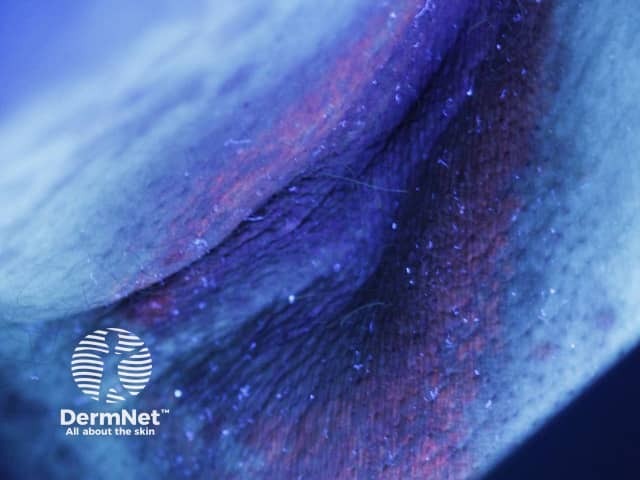
Diagnosis
Treatment
Prevention
Erythrasma is a common skin condition affecting the skin folds under the arms, in the groin and between the toes.
Erythrasma affects males and females, but it is thought to be more common in the groin of males and between the toes of females.
It is reported to be more prevalent in the following circumstances:
The bacteria responsible for erythrasma are gram-positive, non-spore-forming, aerobic or facultative bacilli called Corynebacterium minutissimum.
Erythrasma may coexist with or be confused with other causes of intertrigo including fungal infections such as tinea or Candida albicans (thrush).
Erythrasma presents as well-defined pink or brown patches with fine scaling and superficial fissures. Mild itching may be present.
The common sites for erythrasma are armpits, groin and between the toes. The intergluteal fold, submammary, and periumbilical skin may also be affected. Widespread infections are most often associated with diabetes mellitus.
Erythrasma is classified into three types according to location.


See more images of erythrasma.
Erythrasma is usually self-limiting. It can be complicated by contact dermatitis, lichenification, postinflammatory pigmentation, and coinfection with other bacteria, yeasts, and dermatophytes.
Serious complications are very rare. Corynebacteria have been reported to causes abscess, cellulitis, cutaneous granuloma, endocarditis, pyelonephritis, endophthalmitis, arteriovenous fistula infection and meningitis.
Erythrasma has a typical clinical appearance. Diagnosis may be supported by the following investigations.
Erythrasma can be treated with antiseptic or topical antibiotic such as:
Extensive infection can be treated with oral antibiotics, including erythromycin or tetracycline and usually responds promptly.
Photodynamic therapy using red light (broadband, peaking at 635 nm) has also been used to treat patients with erythrasma.
Recurrence of erythrasma is common. Antibacterial soap can be used to prevent recurrence. Treatment can be repeated if necessary.

