Introduction
Demographics
Causes
Clinical features
Diagnosis
Limits
Other tests
Differential diagnoses
Treatment
Outcome
Appendix: list of 26 fragrances requiring labelling in the EU
Fragrance allergy is an allergic contact dermatitis to a fragrance chemical.
Fragrances and perfumes can either be made from a natural extract or synthesised. They produce a pleasant scent or disguise the unpleasant odour of a product.
Allergy requires prior sensitisation to the fragrance chemical. Subsequent skin contact with the chemical causes a delayed hypersensitivity reaction (type IV) in the hours to days after exposure.
Fragrance allergy is common and is believed to affect around 1% of adults [1]. Rates in children and adolescents are around 1.8%. Fragrance allergy is second only to nickel allergy as a cause of allergic contact dermatitis. However the frequency of relevant positive reactions in dermatology departments is falling due to the reduced use of oakmoss absolute as a fragrance.
Allergic contact dermatitis occurs as frequently in people with and without a history of atopic dermatitis.
Fragrances are not limited to perfumes and cosmetics. They are also found in:
Anyone who uses or is exposed to fragranced products can become sensitised to them over time. Consort allergy is well-recognised.
A European Scientific Committee on Consumer Safety review of fragrances in 2011 listed 82 substances that had been established as contact allergens including 54 synthetic chemicals and 28 natural extracts. Twelve of the chemicals and 8 of the natural extracts were listed as being at high risk of causing sensitisation.
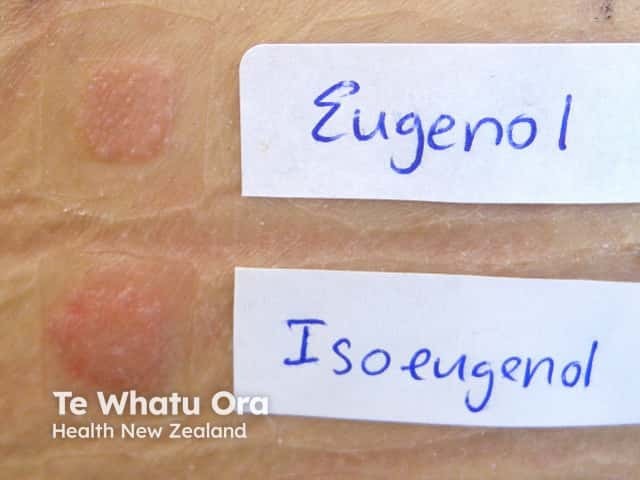
Among the most common are the 15 fragrances that can be identified by patch testing with balsam of Peru, Fragrance Mix I (FM I), and Fragrance Mix II (FM II). Isoeugenol is the most common positive allergen in Fragrance Mix I, and hydroxyisohexyl 3‑cyclohexene carboxaldehyde (Lyral) in Fragrance Mix II.


Fragrance allergy presents as a dermatitis which is often in a streaky pattern where there has been direct contact with the fragrance allergen.
Typically, fragrance allergy presents as scaly erythematous plaques.
Fragrance allergy may affect the mouth (allergic contact stomatitis) resulting in cheilitis, gingivitis, blisters and erosions, or oral lichen planus.
Photoallergy to fragrances has become less common in those countries where the use of musk ambrette has reduced.



A diagnosis of fragrance allergy will typically require a detailed patient history and is confirmed by patch testing.


Patch testing for fragrance allergies usually begins with a baseline series of allergens. These should include balsam of Peru, Fragrance Mix I, and Fragrance Mix II.
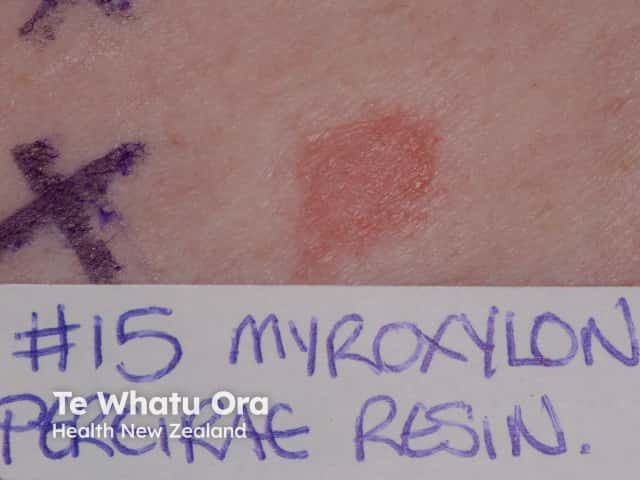
Balsam of Peru is extracted from the Myroxylon pereirae tree. It cross-reacts with other fragrances and a positive reaction occurs in around 50% of patients with fragrance allergy.
Fragrance Mix I can identify 75% of those with fragrance allergy when combined with balsam of Peru. It is a mixture of eight fragrances:
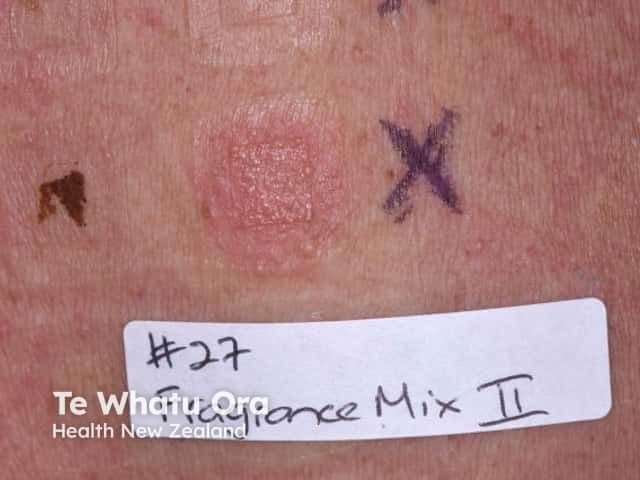
Fragrance Mix II increases the sensitivity of testing as it is a mixture of a further six fragrances:


A patient identified as having a fragrance allergy can be tested with the 26 individual fragrances that require labelling in the European Union. A patient with a positive patch test result to one of the members of the fragrance series can avoid that fragrance by reading labels. See Appendix at the end.
Even if a specific fragrance chemical is identified as causing allergy, it can be difficult to avoid every product that contains it.
It can be futile to test for fragrances that are never labelled since the patient will not be able to identify which products contain the fragrance they have reacted to.
Any leave-on product the patient suspects is causing an allergy can be applied as a customised patch for testing. Patch testing is not suitable for undiluted wash-off products as they are often irritate if left on the skin.
The ‘repeat open application test’ is often more practical and cost-effective than patch testing. Before using a new fragrant leave-on product, the patient applies a dot of the product to the same area of the forearm or inner upper arm twice a day for two weeks. If a rash develops, the product should not be used.
The differential diagnosis for fragrance allergy may include:
Treatment of fragrance allergy requires identification of the allergen followed by avoidance if possible. Treating the allergic contact dermatitis that results from exposure to a fragrance allergen may include:
Fragrances are ubiquitous and avoidance can be a challenge.
The fragrance-allergic patient is best to avoid products that are unlabelled or contain any fragrance.
Select products labelled ‘fragrance-free’ (so-called ‘unscented’ products) but these could still include masking fragrances. Products may contain an unidentified fragrance, for example, if they list ‘botanical’, ‘herbal’, or ‘natural’ ingredients.
The fragrance-allergic patient can use the open application test to screen any new products.
The 26 fragrances in the fragrance series are:

