Introduction
Demographics
Causes
Clinical features
Complications
Diagnosis
Differential diagnoses
Treatment
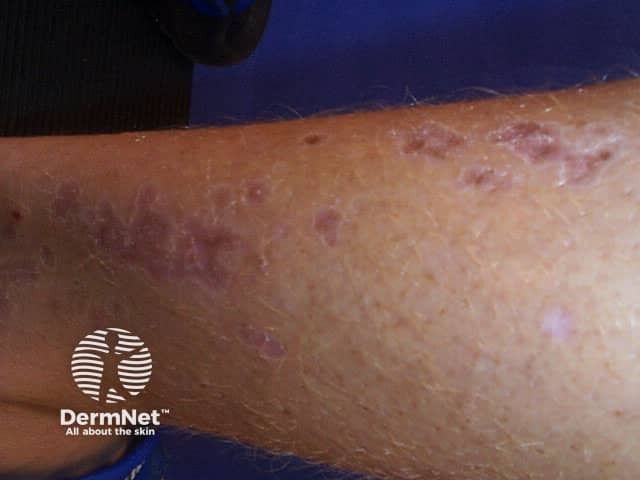
Porokeratosis is a group of skin conditions in which there is abnormal keratinisation. The skin lesions that result are reddish patches (which can be dry or atrophic) with a well-defined ridge-like border called a cornoid lamella [1]. In linear porokeratosis, the lesions are arranged in a linear formation [2].


Linear porokeratosis can be present at birth or not develop until adult life [2].
Like other forms of porokeratosis, the cornoid lamella in linear porokeratosis is due to an expanding proliferation of unusual keratinocytes, which is thought to be due to a genetic mutation. Genetic mutations presenting in the form of mosaicism would explain the linearity and often unilateral distribution of the lesions [3].
Occasionally there is a family history of linear porokeratosis or another kind of porokeratosis, such as disseminated superficial actinic porokeratosis (DSAP), consistent with a genetic predisposition [4].
Linear porokeratosis presents as numerous grouped lesions, each with the characteristic ridge on its border and a central furrow.
They are arranged in one or more lines along a limb or on one side of the trunk, head and neck, following a dermatomal distribution (ie, along the pathway of a sensory nerve).
Localised linear porokeratosis is unilateral and is often confined to a single extremity. The generalised form of linear porokeratosis is rarer, and the lesions affect several extremities and the trunk [5].
The main complication of linear porokeratosis is skin cancer, which can develop within a linear porokeratosis lesion. This may be either a basal cell carcinoma or squamous cell carcinoma and is more likely to occur in older adults [6]. Linear porokeratosis should be monitored for malignancy.
The diagnosis of linear porokeratosis is usually made clinically (based on the appearance), but sometimes a biopsy is needed. The biopsy should include the raised edge of the lesion. The pathology of porokeratosis is very distinct, but it may be necessary to point out the clinical features for the pathologist to find a cornoid lamella within the pathological specimen.
Other linear lesions that should be considered when evaluating linear porokeratosis include:
There is no known cure for linear porokeratosis and treatment is generally disappointing. However, the appearance may improve with the following measures:
Sun protection is very important as exposure to ultraviolet radiation may result in the development of skin cancer within the linear porokeratosis.

