Introduction
Demographics
Causes
Clinical features
Variation in skin types
Complications
Diagnosis
Differential diagnoses
Treatment
Outcome
Pityriasis rosea is a self-limiting rash, which resolves in about 6–10 weeks. It is characterised by a large circular or oval "herald patch", usually found on the chest, abdomen, or back.
The herald patch is followed some time later, typically two weeks or so, by the development of smaller scaly oval red patches, resembling a Christmas tree, distributed mainly on the chest and back.
The exact cause is not known. Viral, bacterial, and non-infective causes have been hypothesised.
Reports suggested pityriasis rosea may be caused by:
Drug-induced reactions
Vaccines
Except for mild to severe itching in up to 25% of patients, no systemic symptoms are typically present during the rash phase of pityriasis rosea. A few days before the rash develops, up to 69% have flu-like symptoms eg, cough or sore throat.
The herald patch is a single patch that appears before the generalised rash of pityriasis rosea. It is a slightly raised, oval, salmon-pink or red plaque 2–5 cm in diameter, with a peripheral scale trailing just inside the edge of the lesion, like a collaret.



See more pityriasis rosea images
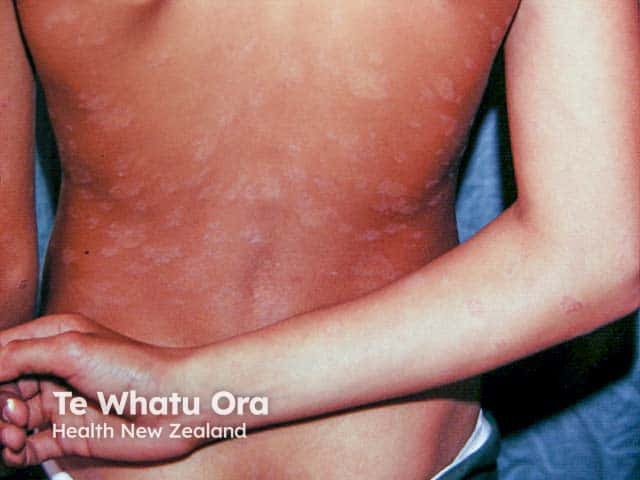
A few days to a few weeks later after the appearance of the herald patch, more scaly patches or plaques appear on the chest and back, most often appearing from the top down. A few plaques may also appear on the thighs, upper arms, and neck, but are uncommon on the face, scalp, palms, or soles.
These secondary lesions tend to be smaller than the herald patch. They are also oval in shape with a dry surface and the long axis of the oval lesion is often orientated around the ribs. Like the herald patch, they may have an inner collaret of scaling. Some plaques may be annular.
Pityriasis rosea patches and plaques usually follow the relaxed skin tension lines or cleavage lines (Langer lines) on both sides of the upper trunk. The rash has been described as looking like a Christmas tree in distribution. Worsening of the rash or a second wave of lesions is not uncommon before eventual spontaneous resolution of the eruption. In children the distribution and lesions are often atypical.


See more pityriasis rosea images
Pityriasis rosea is said to be atypical when diagnosis has been difficult. Atypical pityriasis rosea may be diagnosed when the rash has features such as:
The pityriasis rosea rash often leaves behind patches of lighter (hypopigmented) or darker (hyperpigmented) discolouration. This may be more obvious in darker-skinned people and may take months to return to normal appearance.
In most cases, pityriasis rosea is harmless. However, there are reports of complications such as:
Identification can be challenging at the onset of symptoms. There are no non-invasive tests that confirm the condition. The diagnosis is usually made clinically but may be supported by:
Blood testing for HHV6 (IgG or PCR) is not indicated because nearly 100% of individuals have been infected with the virus in childhood and commercial tests do not currently measure HHV6 activity.
If the diagnosis is uncertain, especially if the palms and soles are affected, it is important to consider the possibility of other conditions.
Clinical features |
Criteria |
||
|---|---|---|---|
Essential |
|
||
Optional |
|
||
Exclusion |
|
||
Source: Zawar V, Chuh A. Applicability of proposed diagnostic criteria of pityriasis rosea:
results of a prospective case-control study in India. Indian J Dermatol. Nov 2013
While pityriasis rosea is a self-limiting disease, an important goal of treatment is to control pruritus, which may be severe in 25% of patients. In addition to education and reassurance, many patients will benefit from:
The following therapies may help with the symptoms and speed up clearance:
Pityriasis rosea will resolve in about 6–10 weeks. Skin discolouration may persist for a few months in darker-skinned people but eventually the skin returns to its normal appearance.
Recurrence of pityriasis rosea outside the acute phase is rare (1–3%), perhaps adding weight to the suggestion that there is long-lasting immunity after a proposed infection. However, a different viral infection may trigger recurrence years later.

