Introduction
Skin conditions can significantly influence psychological and social functioning. People with lesions on the face or hands have particularly high rates of mental health problems.
Stigmatisation, for example where others have avoided touch due to the skin condition, reinforces feelings of shame and can lead to depression and social anxiety. Unfortunately, downplaying this psychosocial burden or suffering in medical settings can lead to worse medical outcomes and poorer quality of life.
Response to acne

What psychosocial problems do skin conditions cause?
Skin conditions can reduce the quality of life, defined by the World Health Organization as a state of complete physical, mental, and social well-being. This can often be attributed to feeling pressured to look normal or comply with social standards.
Many people with a skin condition:
- Experience decreased sense of body image
- Have lower self-esteem
- Avoid situations where the skin is exposed
- Feel anxious about people judging them
- Withdraw from social interactions
- Have sexual and relationship issues
- Feel shame and disgust about their appearance.
Many people who have a visible skin condition at some point will notice a person making an effort not to touch them because of their skin. Experiences like this can have a profound impact and make the individual feel ashamed and also more likely to notice similar events in the future.
Depression in dermatological settings
What is depression?
The psychosocial consequences of having a skin condition can result in depression. Symptoms include:
- Feeling down, low, sad, or tearful
- Loss of pleasure or motivation
- Sleep disturbance, fatigue
- Appetite changes
- Trouble with memory and/or concentration
- Excessive feelings of guilt
- General lack of activity and social engagement
- Suicidal thoughts.
Suicidal thoughts are thoughts like “I wish that one day I just won't wake up” or “Everyone would be better off without me”. These should be taken seriously and help sought from the patient's GP or mental health workers.
How does depression impact skin disorders?
People that have a skin condition and are also depressed may find it especially difficult to adhere to treatment recommendations. Poor adherence may lead to worsening of the skin condition, which may then make their mood even worse.
Depression modulates the perception of itch, ie, people who are depressed may experience worse itch (for example associated with atopic dermatitis). The more severe the depressive symptoms, the more severe itch perception is likely to be. Thus, it is important to target depressive symptoms when treating skin conditions.
Obsessive–compulsive spectrum disorders in dermatological settings
Obsessive–compulsive disorders are far more common in dermatological settings (22%) than in the general public (3.5%).
Compulsive repetitive behaviours can cause or exacerbate skin conditions. These include:
- Scratching (eg, acne excorie)
- Compulsive hand washing causing irritant contact dermatitis
- Hair-pulling (trichotillomania)
- Skin picking (eg, compulsive skin picking).
Some repetitive behaviours can be broken by using distraction techniques e.g. finding another activity to focus attention on when the urge to perform this behaviour occurs. However, in severe cases, it is unlikely that an individual will be able to stop these behaviours without psychological input. These repetitive behaviours often fall outside of conscious awareness, meaning that they can be particularly hard to control.
What is obsessive–compulsive disorder (OCD)?
OCD is characterised by obsessions and compulsions.
- Obsessions are repeated intrusive thoughts, images, or urges.
- Compulsions are repetitive behavioural or mental acts that the individual feels compelled to perform to reduce the distress elicited by the obsessions.
Compulsive behaviours are either not really connected to the desired outcome or the behaviour is excessive and time-consuming. Contamination and cleaning compulsions are common in OCD. These often take the form of repetitive hand washing, bathing, or showering. This can result in skin damage (irritant contact dermatitis) and hence a dermatologic presentation.
The impact of stress on skin conditions
How can stress exacerbate skin conditions?
Cutaneous responses to a sudden stress include:
- Blushing
- Perspiration (excessive perspiration is known as hyperhidrosis).
Long term stress down-regulates immune function, which is one reason why psychological factors impact physical health.
- Major life events are linked to the onset of atopic dermatitis, psoriasis and other chronic skin disorders.
- Everyday life stressors may aggravate symptom severity in the following 24 hours.
- A chronic skin condition is stressful in itself.
This relationship between stress and symptoms can lead to a vicious cycle of somatic symptoms and psychosocial problems.
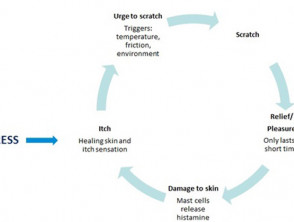
Stress and the itch–scratch cycle
Itch can be elicited by external stimuli (like heat or skin dryness) and by internal stimuli.
- Simply thinking about itch is enough to trigger actual itch sensations.
- Stress modifies the threshold for noticing itch via increased attention (hypervigilance) to sensations and reduced spinal cord inhibition of itch sensations.
Itch leads to scratching, which damages the skin and causes pain, which in turn inhibits itch sensations briefly. Problematic scratching can often lead to feelings of helplessness (in one’s own ability to resist scratching), or guilt (in failing to stop scratching in spite of knowing that it is unhelpful) and therefore to more emotional stress and distress.
Stress and the itch-scratch cycle
Treatment of psychosocial problems
If a skin condition is interfering with the quality of life as described in this article, help is available through either a dermatologist, GP and/or mental health worker. Most of the problems described above can be treated with cognitive behavioural therapy. Medication may also be appropriate for problems like depression, anxiety, and obsessive-compulsive behaviours.