Introduction
Demographics
Causes
Clinical features
Complications
Diagnosis
Treatment
Prevention
Outlook
Seborrhoeic keratosis is a harmless warty spot that appears during adult life as a common sign of skin ageing. Some people have hundreds of them.
Seborrhoeic keratosis (American spelling - seborrheic keratosis) is also called SK, basal cell papilloma, senile wart, brown wart, wisdom wart, or barnacle. The descriptive term, benign keratosis, is a broader term that is used to include the following related scaly skin lesions:



Seborrhoeic keratoses are extremely common. It has been estimated that over 90% of adults over the age of 60 years have one or more of them. They occur in males and females of all races, typically beginning to erupt in the 30s or 40s. They are uncommon under the age of 20 years.
The precise cause of seborrhoeic keratoses is not known.
The name is misleading, because they are not limited to a seborrhoeic distribution (scalp, mid-face, chest, upper back) as in seborrhoeic dermatitis, nor are they formed from sebaceous glands, as is the case with sebaceous hyperplasia, nor are they associated with sebum — which is greasy.
Seborrhoeic keratoses are considered degenerative in nature. As time goes by, seborrhoeic keratoses become more numerous. Some people inherit a tendency to develop a very large number of them. Researchers have noted:
Seborrhoeic keratoses can arise on any area of skin, covered or uncovered, with the exception of palms and soles. They do not arise from mucous membranes.
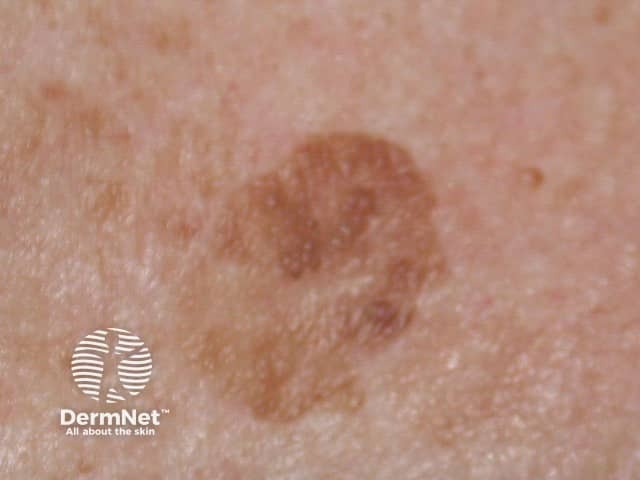
Seborrhoeic keratoses have a highly variable appearance.
They appear to stick on to the skin surface like barnacles.


Variants of seborrhoeic keratoses include:




Seborrhoeic keratoses are not premalignant tumours. However:
Very rarely, eruptive seborrhoeic keratoses may denote an underlying internal malignancy, most often gastric adenocarcinoma. The paraneoplastic syndrome is known as the sign of Leser-Trélat. Eruptive seborrhoeic keratoses that are not associated with cancer are sometimes described as having pseudo-sign of Leser-Trélat.
Eruptive and irritated seborrhoeic keratoses may also arise as an adverse reaction to a medication, such as adalimumab, vemurafenib, dabrafenib, 5-fluorouracil and many chemotherapy drugs.
An irritated seborrhoeic keratosis is an inflamed, red and crusted lesion. It may give rise to eczematous dermatitis around the seborrhoeic keratosis. Dermatitis may also trigger new seborrhoeic keratoses to appear.
The diagnosis of seborrhoeic keratosis is often easy.
Sometimes, seborrhoeic keratosis may resemble skin cancer, such as basal cell carcinoma, squamous cell carcinoma or melanoma.
Dermoscopy often shows a disordered structure in a seborrhoeic keratosis, as is also true for skin cancer. There are diagnostic dermatoscopic clues to seborrhoeic keratosis, such as multiple orange or brown clods (due to keratin in skin surface crevices), white milia-like clods, and curved thick ridges and furrows forming a brain-like or cerebriform pattern.
If doubt remains, a seborrhoeic keratosis may undergo partial shave or punch biopsy or diagnostic excision. [see Seborrhoeic keratosis pathology]
The dominant histopathological features of seborrhoeic keratosis may be described as:
An individual seborrhoeic keratosis can easily be removed if desired. Reasons for removal may be that it is unsightly, itchy, or catches on clothing.
Methods used to remove seborrhoeic keratoses include:
All methods have disadvantages. Treatment-induced loss of pigmentation is a particular issue for dark-skinned patients. There is no easy way to remove multiple lesions on a single occasion.
How to prevent seborrhoeic keratoses is unknown.
Seborrhoeic keratoses tend to persist. From time to time, individual or multiple lesions may remit spontaneously or via the lichenoid keratosis mechanism.
Those associated with dermatitis may regress after it has been controlled.

