Introduction
Atypical target lesions
Targetoid lesions
Diagnosis
A target lesion is a round skin lesion with three concentric colour zones:
Target lesions typically occur in erythema multiforme. They can arise on any body site, including face, upper chest, back, arms, legs, hands, feet and mucous membranes (such as the lips). A target lesion is also called a bulls-eye lesion or a cockade (a rosette pattern of concentric rings).
An iris lesion represents an early target lesion and has two parts:
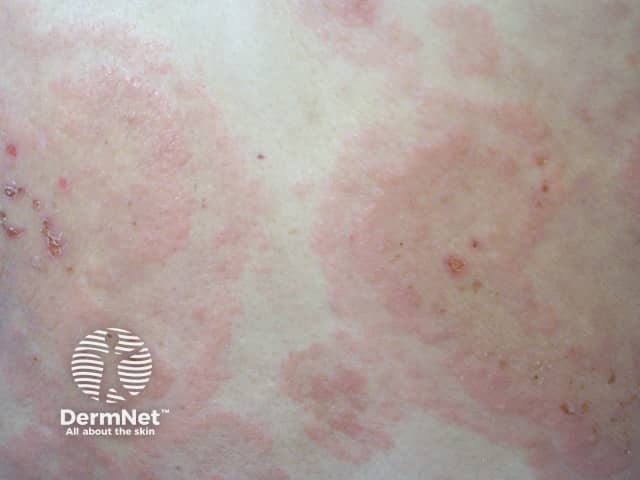
Single-component red plaques are also typical of erythema multiforme.
Target lesions appear within the first 3 days of an episode of erythema multiforme and once one lesion has appeared, it stays in the same location for 7 days or more until the skin heals.



Atypical target lesions show just two zones and/or an indistinct border. In erythema multiforme, these lesions are raised (papular). In Stevens-Johnson syndrome / toxic epidermal necrolysis (SJS/TEN), they are flat (macular).
Targetoid lesions have concentric zones and look similar to target lesions but are not due to erythema multiforme. They may evolve over a different time frame. Several skin conditions cause targetoid lesions.
A targetoid naevus (mole) is also called a cockade naevus (naevus en cocade). They are sometimes multiple. They are usually found on the trunk of a fair-skinned individual but may also be seen in the scalp, particularly in children. They are harmless and tend to remain unchanged long-term. Sometimes the outer, darker rim fades or disappears later in life.



Urticaria is characterised by weals, which are raised plaques with a smooth surface that change location and/or size within a 24 hour period. Weals may be large and have unusual shapes. Targetoid lesions in urticaria have an area of normal skin in the middle surrounded by a raised circular weal. Dermographism (formation of a weal on light stroking of the skin) may be present.



Fixed drug eruption is an adverse drug reaction that usually occurs in the same site/s on the skin every time the medication is taken. A fresh lesion is a well defined targetoid plaque, with a dusky red raised area of skin and sometimes a central blister.
Fixed drug eruption is not usually very extensive. Examination of a skin biopsy by a pathologist may be helpful in making the diagnosis.



Polymorphic light eruption occurs on skin a few hours after it has been exposed to sunlight. As its name suggests, it can take many forms, but generally consists of small or large raised red spots. Targetoid lesions are less common.
Erythema annulare centrifugum begins as a small raised pink spot that enlarges and forms a ring shape, while the central area flattens and clears. There may be an inner rim of scale, resulting in the 3 zones characterising a targetoid lesion.

Subacute cutaneous lupus erythematosus occurs on the upper back and chest, often following sun exposure. It often has a ring-shaped appearance (annular or polycyclic), and occasionally develops a targetoid lesion with 3 concentric zones.
Rowell syndrome is a rare form of lupus erythematosus with targetoid lesions and positive blood tests for lupus antibodies (a speckled pattern of antinuclear antibodies, and sometimes positive anti-La/anti-Ro or rheumatoid factor). The skin lesions are large, raised and ring-shaped. Patients may also have chilblains.
Polymorphic eruption of pregnancy (PUPPP) occurs in the last 3 months of pregnancy. In most women, pink papules develop within the stretch marks on the abdomen. These may be surrounded by a pale halo or evolve to targetoid lesions with 3 rings. Polymorphic eruption of pregnancy is characteristically very itchy.
Targetoid lesions may occur in several bullous (blister-forming) disorders, including:
The targetoid lesions of linear IgA bullous disease have peripheral blisters, in contrast to target lesions in erythema multiforme, which have central blisters.


Some forms of vasculitis may present with targetoid lesions on the skin. These include:



The impact of a ball, such as a squash ball or a table tennis ball, hitting the skin at high speed can also produce a targetoid bruise.
Another name for a hobnail haemangioma is targetoid haemosiderotic haemangioma. It is a benign (non-cancerous) overgrowth of blood vessels, generally occurring on an arm, leg or trunk of a young to middle-aged person. It typically has a small red/purple raised centre surrounded by a purple or brown ring that can expand or disappear altogether.
As targetoid lesions are descriptive rather than diagnostic, a careful medical history and full skin examination are necessary to make the correct diagnosis.
Consider the time course of development, drug history, and total number and type of skin lesions. A skin biopsy can often help to distinguish these disorders.

