Introduction
Neurocutaneous disorders
Neuropsychiatric and addiction disorders
Disorders related to drug abuse
Neuropathic itch
Neurological diseases associated with skin signs include:
Neuropathic itch is also discussed in this topic.
Neurocutaneous disorders are a group of congenital multisystem diseases that result in the growth of tumours in the brain, spinal cord, skin and other organs.
Tuberous sclerosis complex (TSC) is an autosomal dominant syndrome caused by mutations in the tumour suppressor genes, TSC1 and TSC2. Diagnosis of TSC is based on major and minor clinical criteria. Major features have higher specificity for TSC than minor features. Note that there is no single diagnostic feature, and none are specific for TSC.
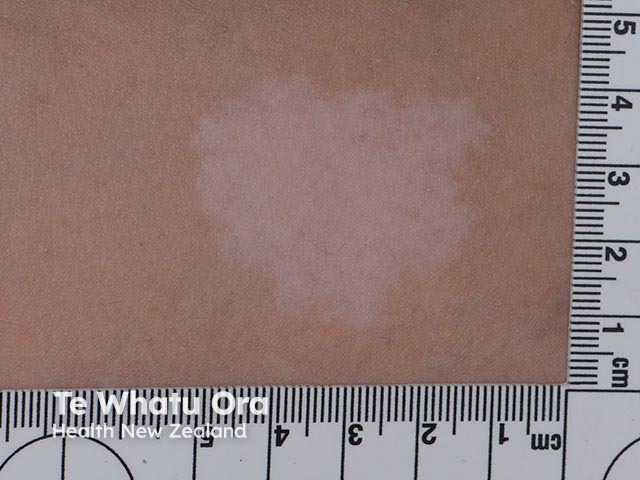
Skin manifestations of tuberous sclerosis include:
Other clinical manifestations include retinal nodular hamartomas, and lesions in the kidneys (angiomyolipomas), heart (rhabdomyomas) and brain (subependymal giant cell astrocytomas, cortical tubers). Patients often have learning and behavioural difficulties and seizures.


Neurofibromatosis is an autosomal dominant condition with three distinct clinical subtypes:
Similar to tuberous sclerosis, patients with neurofibromatosis can have learning difficulties.
Cutaneous features of NF1 include:
Cutaneous features of NF2 include:
Non-cutaneous features of NF1 and NF2 include:
Features of schwannomatosis include:



Also known as Louis-Bar syndrome, ataxia-telangiectasia is a rare autosomal recessive disorder that affects the central and peripheral nervous systems. Ataxia (unsteady gait) is often the earliest clinical manifestation of this condition.
Cutaneous telangiectasias (spidery blood vessels) develop after the age of 3 years. They begin in the corners of the eye (ocular canthus) and spread to the membrane covering the eye (bulbar conjunctiva). Telangiectasias may later develop on the cheeks, ears, eyelids, chest, and skin folds of knees and elbows.
Other cutaneous features of ataxia-telangiectasia include:
Non-cutaneous features of ataxia-telangiectasia include:
Sturge–Weber syndrome is a rare disorder that involves vascular malformations affecting the face and eye, which correspond with a leptomeningeal angioma, a vascular tumour in the brain. This often causes corresponding neurological and ocular deficits.
Neurological features are progressive and can include seizures, focal neurological deficits and intellectual disability. Visual field defects are also common if the occipital cortex of the brain is involved.

Psychiatric disorders are central nervous system conditions with a neurobiological basis. They generally involve disturbances of emotion, cognition, motivation and socialisation. Psychiatric disorders can either lead to psychocutaneous (skin) manifestations as a consequence or they may arise as a result of a chronic dermatological condition that impacts on the patient’s mental health.
There are four main types of primary psychocutaneous diseases.
A delusional disorder may present as delusions of parasitosis.
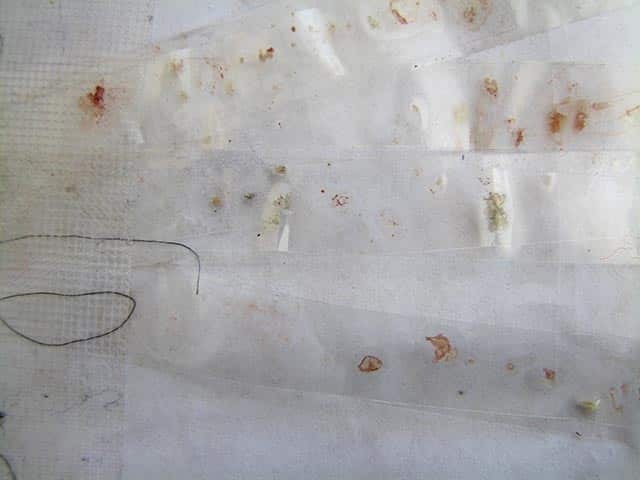
A factitious disorder may present as dermatitis artefacta.



Somatic symptom disorder (previously known as a somatoform disorder) may present as cutaneous dysaesthesia.
A compulsive disorder may present as obsessive–compulsive disorder (OCD).



The use and abuse of drugs may cause cutaneous manifestations and skin disease as a result of local and systemic toxic effects from the drugs involved.







Pruritus (itch) can originate from anywhere in the nervous system. Examples of conditions associated with neuropathic itch include:




